Pelvis / Uterus / MRI
torsion-2
Acute presentation of severe pelvic pain, often with nausea/vomiting, in a woman of reproductive age. MRI may be requested when diagnosis is initially missed or to evaluate an adnexal mass in the setting of acute pain.
Key Images
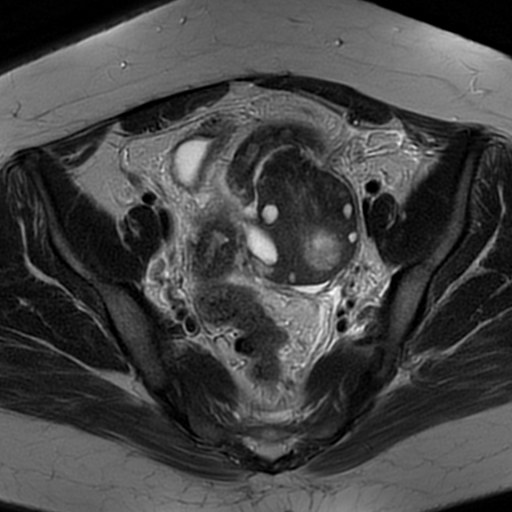
Torsion-2 01
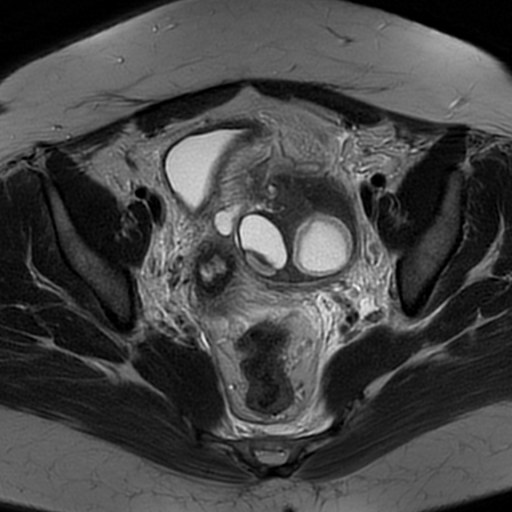
Torsion-2 02

Torsion-2 03
Look For First
- Enlarged ovary (>5 cm maximum diameter) with rounded/spherical morphology and central edema
- Ovary shifted toward midline anterior or posterior to uterus, with uterine deviation toward the torsed side
- Twisted vascular pedicle appearing as a 'whirlpool' structure between uterus and ovary
Key MRI Findings
- T1 weighted imaging may demonstrate a thin rim of high signal intensity (methemoglobin) indicating hemorrhage within the torsed ovary.
- T2 weighted imaging often shows low signal intensity due to interstitial hemorrhage and edema, with follicles displaced peripherally by central stromal edema.
- T1 post-gadolinium imaging reveals reduced or absent contrast enhancement of the torsed ovary, reflecting vascular compromise and ischemia.
- The torsed ovary demonstrates edematous swelling with maximum diameter typically >5 cm (89% sensitive), often with a more spherical configuration than the normal bean-shaped ovary.
- Distension of the fallopian tube on the affected side may be present, indicating tube involvement in the torsion.
- Free peritoneal fluid may be visualized, reflecting the acute inflammatory process and potential hemorrhage.
- The characteristic 'whirlpool' sign shows layered twisting of the fallopian tube, mesosalpinx, and vascular pedicle between the uterus and ovary.
- Associated ovarian mass or cyst (corpus luteum, teratoma, or functional cyst) is present in >85% of cases and may be the nidus for torsion.
Differential Diagnosis
- Ectopic pregnancy: positive beta HCG and characteristic gestational sac location; ovary typically normal size without edema.
- Ruptured ovarian cyst: abrupt midcycle pain with free fluid/hemoperitoneum but ovary returns to normal size without persistent edema.
- Pelvic inflammatory disease: more indolent disease course with bilateral salpingitis and endometritis; ovaries normal size.
- Massive ovarian edema from malignant lymphatic obstruction: lack of torsion history and absent whirlpool sign; typically bilateral.
- Degenerating pedunculated leiomyoma: uterine location with heterogeneous signal; no ovarian enlargement or whirlpool sign.
- Appendicitis: inflamed appendix visualized separately; ovaries normal without edema or displacement.
Discussion
- The diagnosis of adnexal torsion is commonly missed clinically, leading to delayed surgery and increased risk of ovarian infarction within hours of onset.
- Venous and lymphatic obstruction from twisting causes central ovarian edema that further compromises arterial inflow, creating a self-perpetuating cycle of ischemia.
- Over 85% of torsion cases are associated with ovarian enlargement from a mass or cyst; corpus luteum and mature cystic teratomas are the most common predisposing lesions.
- Hemorrhagic infarction can develop rapidly, and imaging delay allows progression from viable (non-friable, blue/black appearance) to necrotic ovary.
- The presence of blood flow on Doppler does not exclude torsion, while absence of flow is highly specific but may not be readily apparent on MRI.
- An ovarian mass presenting acutely with severe pain is suspicious for torsion, as masses are rarely painful unless complicated by torsion, rupture, or hemorrhage.
Prenuvo Reporting Pearl
In whole-body screening MRI, note any enlarged ovary (>5 cm) with central edema and rounded shape; if acute symptoms are present, describe the whirlpool sign and degree of enhancement to alert clinicians to possible torsion requiring urgent surgery.
Pitfalls
- Misinterpreting central edema and follicular displacement as a primary ovarian mass rather than recognizing this as the hallmark sign of torsion.
- Assuming normal or preserved Doppler flow excludes torsion; venous obstruction can occur with partially preserved arterial flow.
- Failing to recognize the whirlpool sign due to lack of awareness of its appearance; it is specific but requires careful inspection of the vascular pedicle.
- Attributing an enlarged, edematous ovary with an associated mass solely to the mass effect without considering torsion as a complication, especially in the setting of acute pain.