Pelvis / Uterus / MRI
Incarcerated right femoral hernia
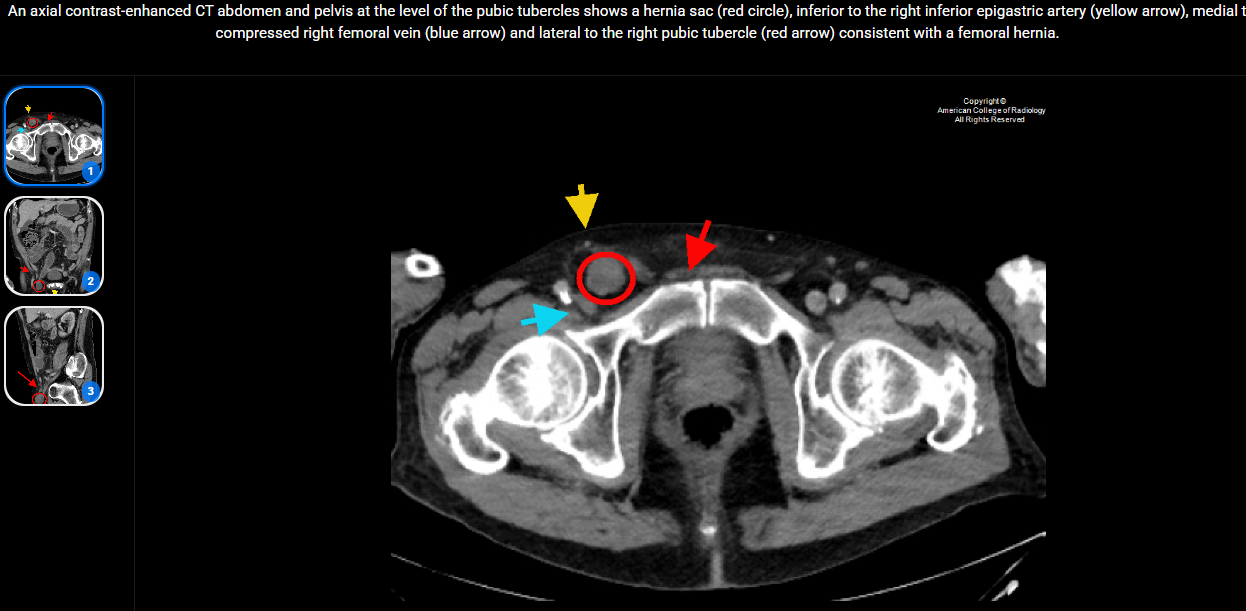
Incarcerated femoral hernia presenting with groin pain and palpable mass.
Clinical indication is to evaluate for herniation and assess for signs of strangulation that would require urgent surgical intervention.
Key Images
Image
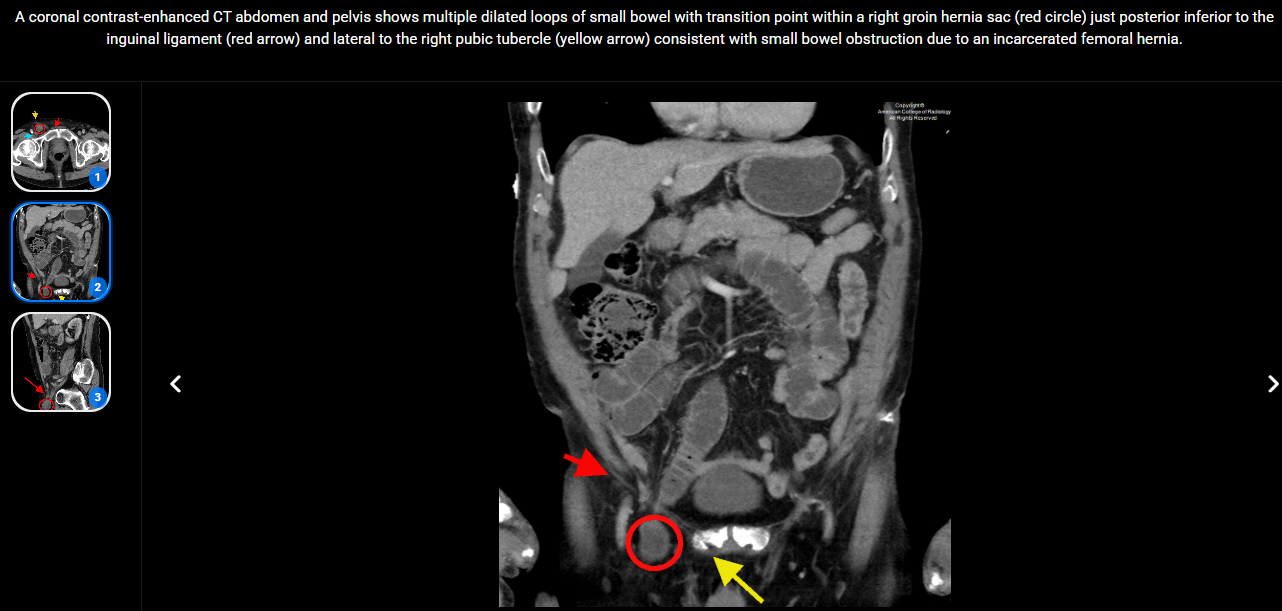
Image 2
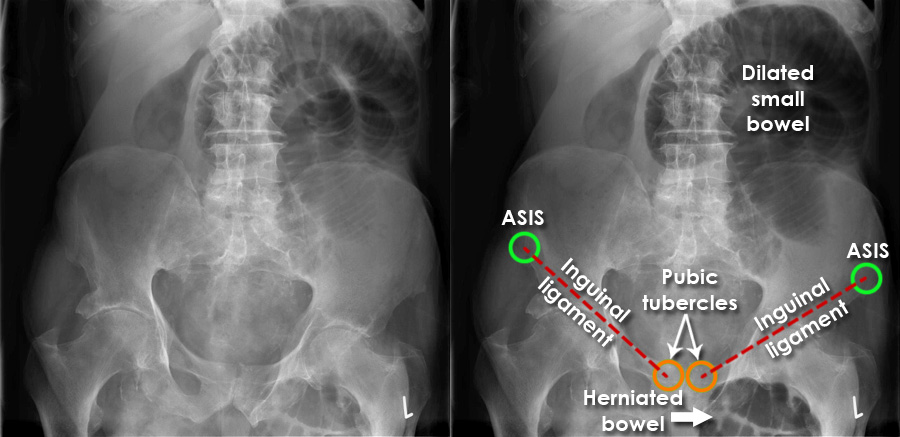
Image 3
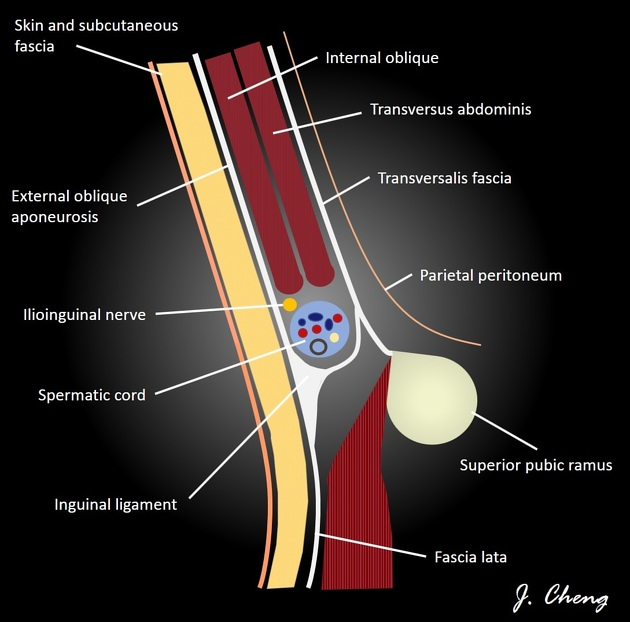
A sagittal schematic of the male inguinal canal demonstrating its boundaries and relations.
Case Discussion
Due to its oblique course through multiple layers of fascia, the walls of the inguinal canal can be difficult to conceptualise. This diagram attempts to simplify the boundaries and structures within the canal. This diagram pertains to males; however, in females the spermatic cord will be replaced by the round ligament.
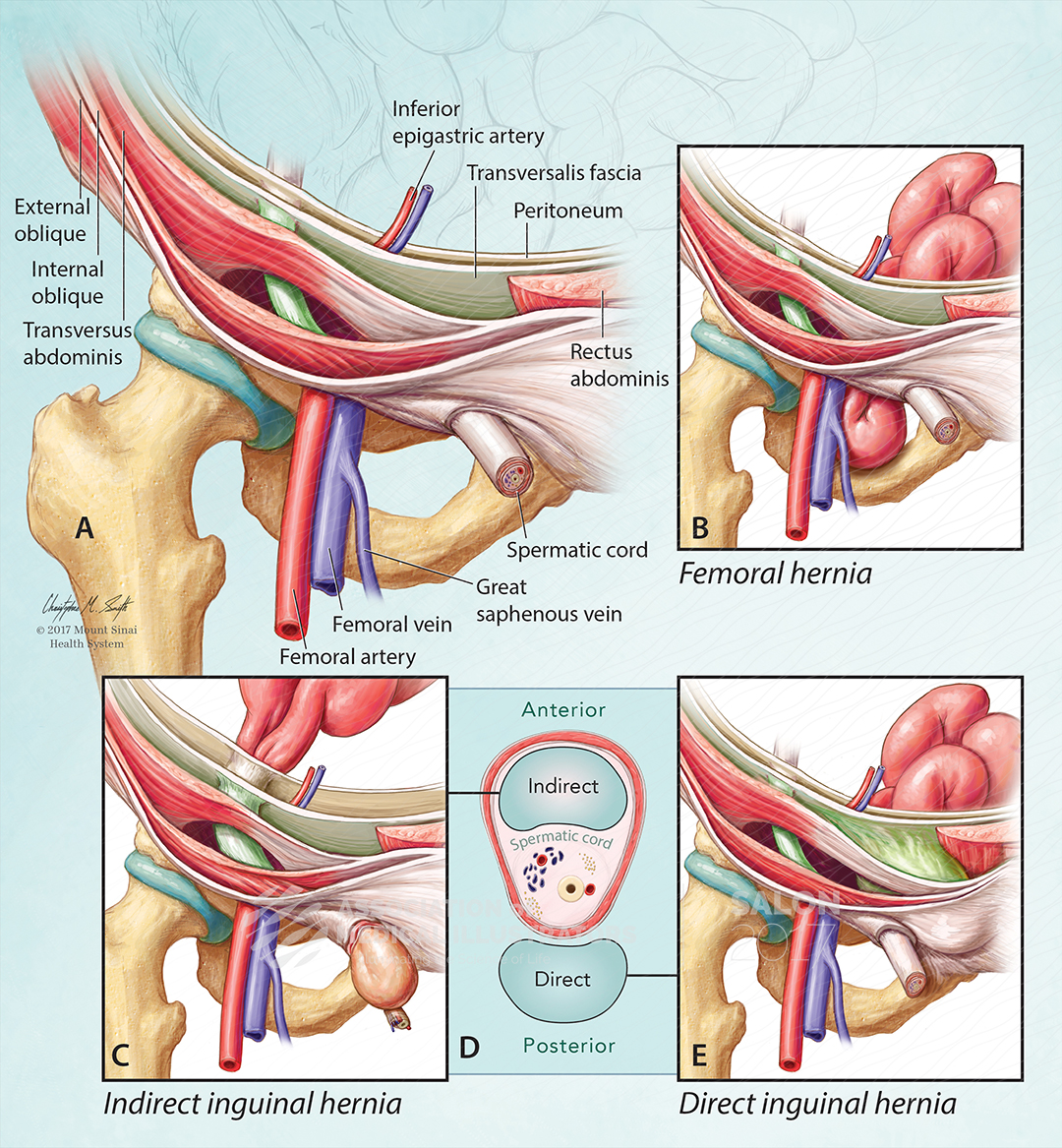
Image 5
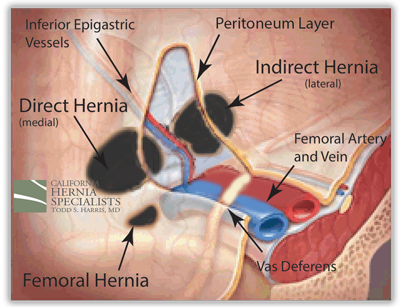
Image 6
Look For First
- Hernia sac located lateral to the pubic tubercle and medial to the femoral vein
- Mass effect compressing or displacing the femoral vein medially
- Hernia sac positioned inferior to the inguinal ligament (posterior/inferior course) rather than anterior to it
Key Image Findings
- Femoral hernia appears as a focal sac located lateral to the pubic tubercle, distinguishing it from medial inguinal hernias.
- The hernia sac is positioned medial to the femoral vein, which may show mass effect and compression due to the expanding hernia.
- The sac is located inferior to both the inferior epigastric artery and the inguinal ligament, passing posterior and inferior to the ligament rather than anterior as in inguinal hernias.
- On cross-sectional imaging (CT), the hernia sac can be traced into the femoral canal through the femoral ring defect.
- Incarcerated femoral hernias show a transition zone where bowel herniates through the rigid femoral ring, with potential crowding and compression of contents.
- Signs of strangulation include bowel wall thickening, reduced enhancement, mesenteric edema, and free fluid around the herniated loops.
- The narrow diameter of the femoral ring increases risk of bowel becoming trapped and irreducible.
- Associated findings may include ascites or other causes of increased intra-abdominal pressure (e.g., chronic cough from COPD, bladder outlet obstruction).
Differential Diagnosis
- Incarcerated indirect inguinal hernia: hernia sac courses anterior to the inguinal ligament and lateral to the inferior epigastric artery, arising from the internal ring.
- Incarcerated direct inguinal hernia: hernia sac is medial to the inferior epigastric artery, protrudes through Hesselbach's triangle, and courses anterior to the inguinal ligament.
- Femoral lymphadenopathy: appears as rounded nodes without a sac or connection to intra-abdominal contents; lacks mass effect on the femoral vein.
- Femoral artery pseudoaneurysm: enhances briskly with contrast and communicates with the femoral artery lumen; no herniated visceral contents.
- Lipoma or other soft tissue mass: lacks the characteristic anatomical relationship to the pubic tubercle, femoral vein, and inguinal ligament.
- Hydrocele or fluid collection: confined to the inguinal canal or scrotum; no relationship to the femoral ring or canal.
Discussion
Direct, indirect, and femoral hernias are all groin-region hernias but differ in their anatomic path, relation to the inferior epigastric vessels, and typical patient profile. radiopaedia
Direct inguinal hernia
- Protrusion of abdominal contents through a weakness in the posterior wall of the inguinal canal within Hesselbach’s triangle. radiopaedia
- Lies medial to the inferior epigastric vessels. teachmeanatomy
- Typically acquired, related to weakening of transversalis fascia and chronic raised intra‑abdominal pressure (e.g., COPD, constipation, bladder outlet obstruction). radiopaedia
- More common in older men; often bilateral; less likely to extend into scrotum or to strangulate due to a wider neck. teachmeanatomy
- Presents as a reducible groin bulge that enlarges with coughing/straining, usually above the inguinal ligament. radiopaedia
Indirect inguinal hernia
- Herniation of abdominal contents through the deep inguinal ring into the inguinal canal, following the course of the processus vaginalis. buoyhealth
- Lies lateral to the inferior epigastric vessels. teachmeanatomy
- Often congenital due to a patent processus vaginalis; more common in younger patients, including children. verywellhealth
- Can track into the scrotum or labia majora, more prone to incarceration/strangulation than direct hernias. buoyhealth
- Clinically appears as a groin or scrotal mass that increases with Valsalva and may be irreducible if incarcerated. verywellhealth
Femoral hernia
- Protrusion of abdominal contents through the femoral canal, just below the inguinal ligament, medial to the femoral vein. ncbi.nlm.nih
- Presents as a bulge in the upper thigh or groin, inferolateral to the pubic tubercle and below the inguinal ligament. quality.healthfinder.fl
- More common in women due to a wider pelvis; often small but with a narrow neck. en.wikipedia
- High risk of incarceration and strangulation, frequently presenting as an emergency. teachmesurgery
- Surgical repair recommended once diagnosed, often with mesh; approach may be open, laparoscopic, or robotic. my.clevelandclinic
- Do you want a similarly brief bullet outline focused specifically on exam-style differentiating features (surface landmarks, neck position, risk of strangulation)?
Reporting Pearls
Describe the hernia sac location using the anatomical triangle: identify it as lateral to the pubic tubercle, medial to the femoral vein (note any compression), and inferior to the inguinal ligament. Specify whether contents appear incarcerated or strangulated based on wall enhancement and surrounding edema, and communicate urgency if strangulation features are present.
Pitfalls
- Misidentifying a femoral hernia as an inguinal hernia by failing to note the posterior/inferior course relative to the inguinal ligament; inguinal hernias course anterior to the ligament.
- Overlooking femoral hernias in males, who are less commonly affected but remain at risk with chronic pressure-increasing conditions.
- Failing to assess for signs of strangulation such as bowel wall thickening, reduced enhancement, mesenteric fat stranding, or free fluid, which necessitate urgent surgery.
- Confusing femoral hernias with femoral lymphadenopathy or other femoral space masses that lack the characteristic sac configuration and hernia contents.