Astrocytoma (IDH-mutant with 1p19q non-codeletion status)
Key Images
Look For First
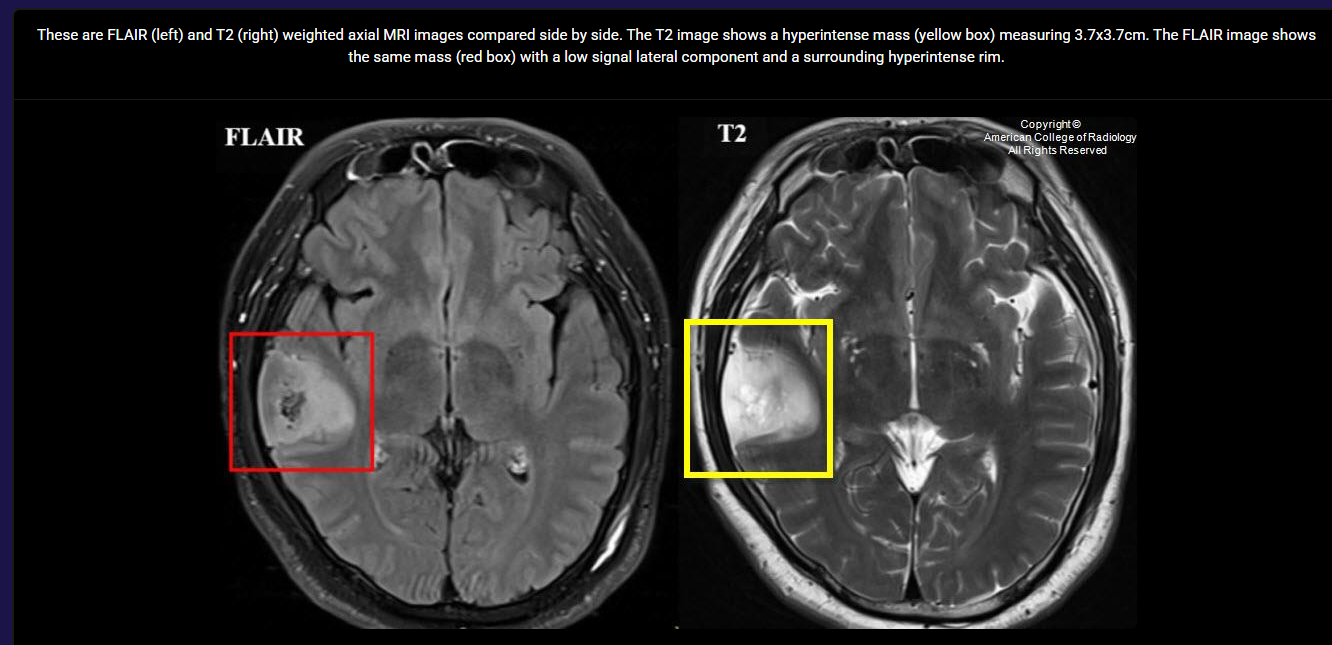
- T2-FLAIR mismatch sign: hyperintense lesion on T2-weighted imaging with hypointense center on FLAIR sequences
- Supratentorial location with predilection for frontal and temporal lobes
- Hyperintense rim surrounding the T2-FLAIR mismatch region
Key Image Findings
- T2-FLAIR mismatch sign is highly specific (though low sensitivity) for IDH-mutant astrocytoma without 1p19q codeletion, with positive predictive value up to 83%.
- Lesion demonstrates hyperintensity on T2-weighted MRI sequences combined with hypointensity on FLAIR sequences in the same region.
- Hyperintense rim of FLAIR signal surrounding the central area of mismatch is a characteristic feature of this tumor subtype.
- Supratentorial location with frequent involvement of frontal and temporal lobes is typical for these tumors.
- T2-FLAIR mismatch sign does not correlate with tumor grade and is not present in all cases of these astrocytomas.
- The imaging pattern reflects the specific molecular and histological characteristics of IDH-mutant, 1p19q non-codeleted astrocytomas.
Differential Diagnosis
- IDH-mutant oligodendroglioma with 1p19q codeletion: typically lacks the T2-FLAIR mismatch sign; molecular testing (1p19q codeletion status) is definitive distinguishing feature.
- IDH wild-type glioblastoma: typically shows higher grade features with greater enhancement and mass effect; lack of T2-FLAIR mismatch sign; molecular testing confirms IDH wild-type status.
- Metastatic disease: usually multiple lesions with distinct enhancement patterns, located at gray-white matter junction; clinical history of extracranial primary malignancy.
- Low-grade pilocytic astrocytoma: typically occurs in cerebellum or optic pathway in younger patients; different molecular profile; less infiltrative appearance.
- Dysembryoplastic neuroepithelial tumor (DNET): typically small, cortical lesion with 'bubbly' appearance; less infiltrative; seizures are common presentation.
Discussion
T2-FLAIR mismatch sign is a crucial imaging biomarker with high specificity for IDH-mutant astrocytomas lacking 1p19q codeletion, enabling confident radiological diagnosis when present.
The sign's high specificity (but low sensitivity) means its presence is strongly indicative of this tumor subtype, though absence does not exclude it.
IDH mutation status and 1p19q codeletion status are molecular characteristics that fundamentally define tumor classification and prognosis according to current WHO criteria.
Young adult demographic (20-45 years) with seizure presentation should prompt careful evaluation for supratentorial glioma in frontal or temporal lobes.
Definitive diagnosis requires integration of imaging findings with molecular and histological analysis; imaging alone cannot confirm tumor subtype.
Surgical resection is the primary treatment goal, with prognosis dependent on tumor grade, type, and extent of resection.
Reporting Pearls
When reporting IDH-mutant astrocytoma without 1p19q codeletion, specifically describe the T2-FLAIR mismatch sign as: 'T2-hyperintense, FLAIR-hypointense lesion with hyperintense FLAIR rim at [location], highly suggestive of IDH-mutant astrocytoma; molecular confirmation recommended.' This precise language alerts clinicians to the specific molecular subtype while emphasizing the need for confirmatory testing.
Pitfalls
- Assuming absence of T2-FLAIR mismatch sign excludes IDH-mutant astrocytoma without 1p19q codeletion; the sign has low sensitivity, so negative imaging does not rule out the diagnosis.
- Overinterpreting T2-FLAIR mismatch sign as indicative of tumor grade; the sign reflects molecular characteristics, not WHO grade.
- Failing to distinguish from IDH-mutant oligodendroglioma with 1p19q codeletion based on imaging alone; molecular testing is mandatory for definitive classification.
- Misidentifying the FLAIR hyperintense rim as edema rather than part of the pathological mismatch sign; the rim is integral to the characteristic imaging pattern.