Proliferating trichilemmal cyst
Key Images


Look For First
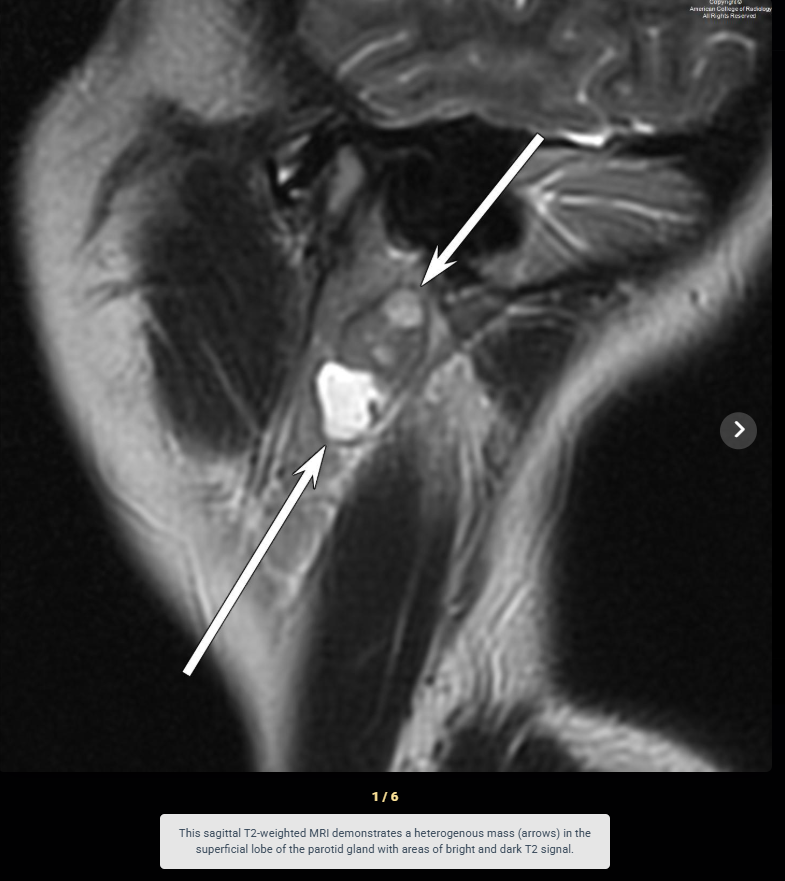
- Heterogeneous T2 signal intensity within a well-circumscribed mass
- Heterogeneous enhancement with wall enhancement and mural nodules
- Lobulated contour with areas of high T1 signal suggesting protein-rich keratin content
Key Image Findings
- On T2-weighted MRI, proliferating trichilemmal cysts demonstrate heterogeneous signal intensity, reflecting mixed solid epithelial proliferation and cystic keratin-filled components.
- T1-weighted imaging typically shows homogeneous or heterogeneous intrinsic signal with characteristic areas of high T1 signal corresponding to protein-rich eosinophilic keratin.
- Post-contrast T1-weighted MRI reveals variable wall enhancement with mural nodules of differing thicknesses, correlating histopathologically with solid epithelial lobules and cystic cavities.
- On CT, lesions appear as poorly-enhancing, well-circumscribed, hypodense masses with smooth borders and may display circular mineralization patterns from layered, protein-rich cystic material.
- Lesions typically present as well-defined, smooth-bordered masses in the skin or superficial soft tissues, with 90% arising on the scalp; extracutaneous presentation in parotid region is unusual.
- Features suggesting potential malignant transformation include size greater than 5 cm, rapid growth, irregular borders, and invasion into adjacent structures.
- Proliferating trichilemmal cysts represent epithelial proliferation occurring in approximately 2% of simple trichilemmal cysts, characterized histologically by variable squamous epithelial proliferation, cellular atypia, and mitotic figures.
Differential Diagnosis
- Pleomorphic adenoma: distinguished by presence of extremely high T2 signal regions, mixed solid and cystic components on MRI, and typical location in parotid gland; however, heterogeneous enhancement and mural nodules can mimic proliferating trichilemmal cyst.
- Simple trichilemmal cyst: lacks epithelial proliferation and cellular atypia on histology; typically homogeneous on MRI and does not show the same degree of enhancement or mural nodularity.
- Well-differentiated mucoepidermoid carcinoma: distinguished by different histopathologic appearance with mucous, intermediate, and squamous cells; typically shows more aggressive imaging features.
- Dermoid cyst: usually contains fat and may show higher T1 signal from fat; lacks the protein-rich keratin layering and heterogeneous enhancement pattern of proliferating trichilemmal cysts.
- Epidermoid cyst: demonstrates restricted diffusion on DWI and typically shows homogeneous T2 signal; lacks the mural enhancement and nodularity seen in proliferating trichilemmal cysts.
Discussion
Proliferating trichilemmal cysts arise from the outer root sheath of hair follicles and undergo epithelial proliferation with cellular atypia in approximately 2% of cases, distinguishing them from simple benign trichilemmal cysts.
Aso known as pilar cysts, are benign accumulations of keratin along the outer hair root sheath, most commonly on the scalp. They are the most common subcutaneous nodule incidentally found on head imaging and are of no clinical relevance when asymptomatic 1. Uncommonly, they can develop into the neoplastic form known as proliferating trichilemmal cysts, which can be locally aggressive.
Although usually benign, proliferating trichilemmal cysts can grow large, ulcerate, and rarely undergo malignant transformation with potential for metastases, making size and growth rate important imaging parameters to monitor.
The heterogeneous appearance on cross-sectional imaging reflects the mixed pathology of solid epithelial lobules, irregular proliferating regions, and cystic keratin-filled cavities.
Presentation in unusual locations such as the parotid gland warrants cross-sectional imaging to exclude other diagnoses and evaluate extent of involvement, as 90% of trichilemmal cysts are cutaneous scalp lesions.
Complete surgical excision including a margin of normal tissue around the capsule is essential for both simple trichilemmal cysts and proliferating variants to minimize recurrence risk.
Histopathological examination is required to definitively diagnose proliferating trichilemmal cysts and distinguish benign forms from those with cytologic atypia that may indicate malignant potential.
Reporting Pearls
Describe proliferating trichilemmal cysts as a heterogeneous, well-circumscribed mass with variable T2 signal intensity, areas of T1 hyperintensity, and variable wall enhancement with mural nodules; note the size (particularly if >5 cm), growth pattern, and relationship to adjacent structures to assess for malignant features.
Pitfalls
- Heterogeneous enhancement with mural nodules can be mistaken for pleomorphic adenoma, particularly when the lesion arises in the parotid region; correlation with T2 signal heterogeneity and high T1 signal from keratin can help distinguish the lesions.
- Unusually large lesions or those with irregular borders and invasion into surrounding soft tissues may be falsely attributed to malignancy; histopathology is required to confirm malignant transformation.
- Simple trichilemmal cysts with mild heterogeneity may be overcalled as proliferating variants; lack of cellular atypia and mitotic figures on histology distinguishes simple from proliferating cysts.
- Extracutaneous presentation in deep soft tissues such as the parotid gland may lead to diagnostic confusion with primary salivary gland tumors; clinical history of superficial origin or prior cutaneous pathology is helpful.