Incidental Adnexal Cystic Lesions on CT/MRI
Reference Images
Initial Triage
First question
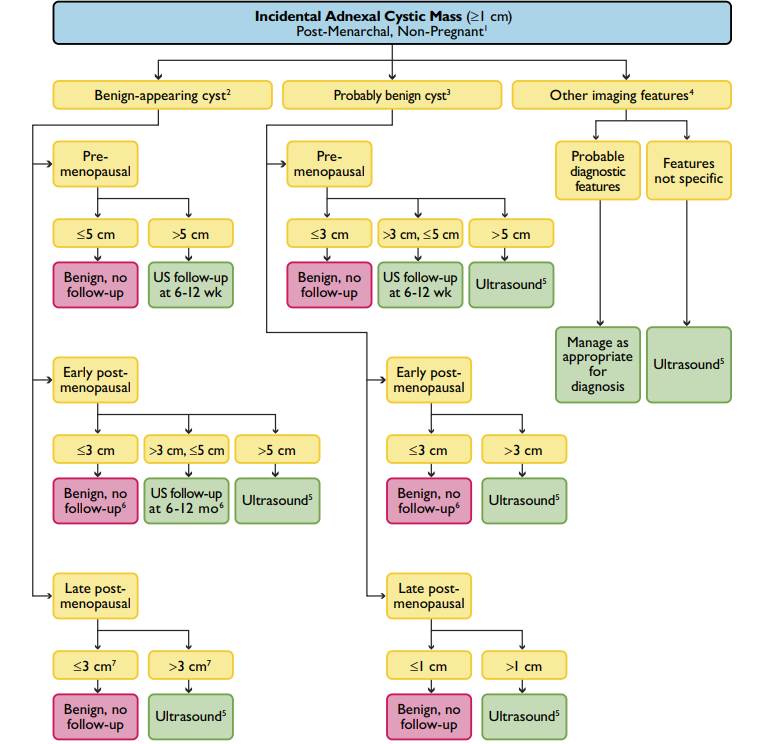
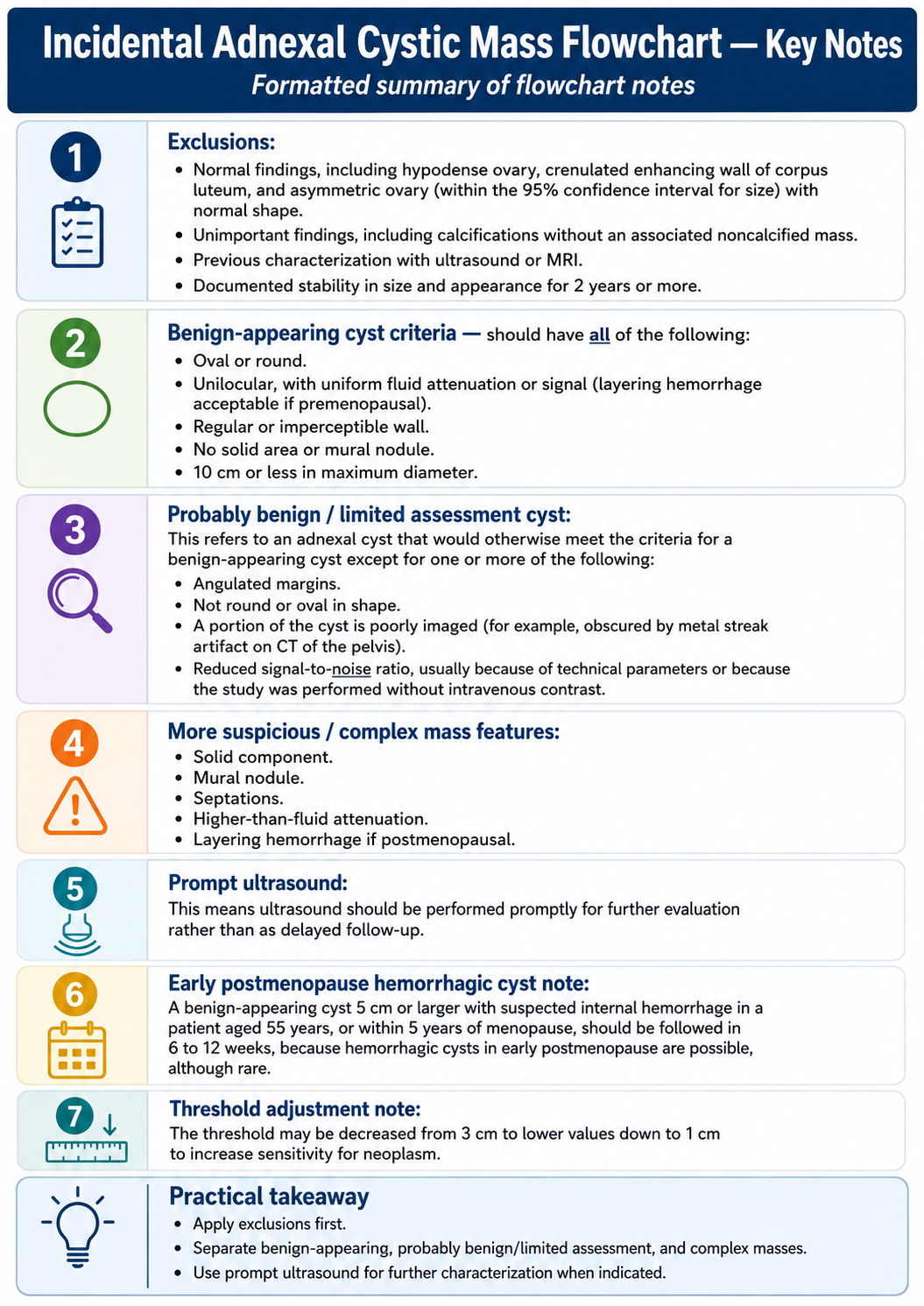
Apply only to nonpregnant, average-risk, asymptomatic post-menarchal patients with incidental CT/MRI findings.
Exclude first
- Normal findings, crenulated enhancing corpus luteum, asymmetric but normal-size ovary, or calcification without a noncalcified mass.
- Previously characterized by ultrasound/MRI or stable in size and appearance for 2 years or more.
- If the mass is not fully seen or characterization is limited, recommend pelvic ultrasound or dedicated pelvic MRI.
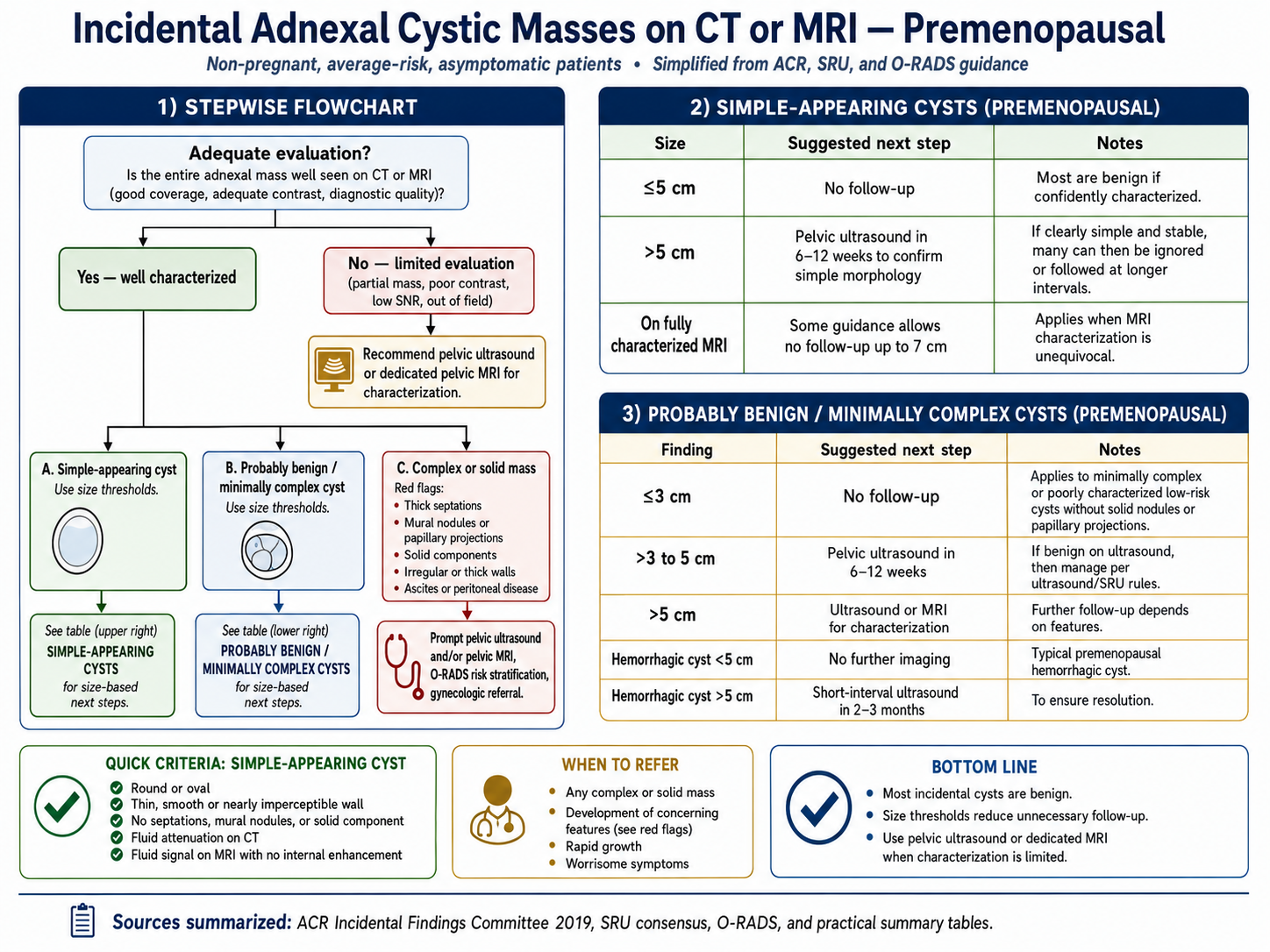
Simple-appearing cyst
- Round or oval, unilocular, fluid attenuation/signal, thin smooth wall, and no solid component or mural nodule.
- Layering hemorrhage can still be acceptable in a premenopausal patient.
Size Thresholds
Premenopausal
- Simple cyst 5 cm or smaller: no follow-up.
- Simple cyst larger than 5 cm: pelvic ultrasound in 6-12 weeks to confirm simple morphology.
- Fully characterized MRI may allow no follow-up up to about 7 cm when unequivocally simple.
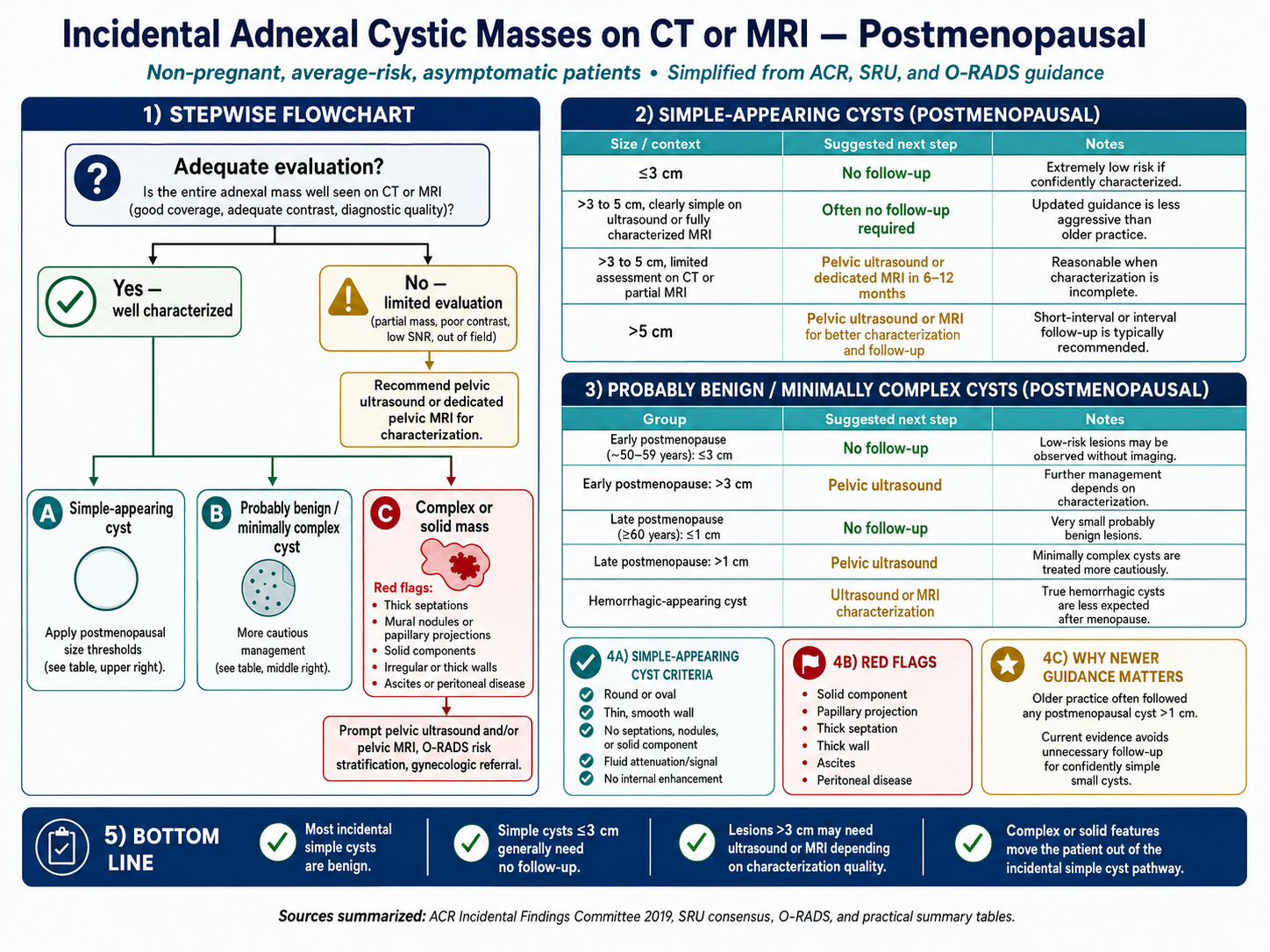
Postmenopausal
- Simple cyst 3 cm or smaller: no follow-up.
- Simple cyst 3-5 cm: no follow-up if confidently simple on ultrasound or fully characterized MRI; otherwise pelvic US or MRI in 6-12 months.
- Simple cyst larger than 5 cm: pelvic ultrasound or MRI for characterization and interval follow-up.
Complex / Limited
Probably benign / limited
- Minimally complex or poorly characterized cysts without solid nodule or papillary projection use lower thresholds.
- Premenopausal: 3 cm or smaller often no follow-up; 3-5 cm pelvic US in 6-12 weeks; larger than 5 cm US or MRI.
- Postmenopausal: early postmenopause uses about 3 cm as a no-follow-up threshold; late postmenopause uses about 1 cm.
Red flags
- Thick septations, mural nodules, papillary projections, solid component, irregular/thick wall, ascites, or peritoneal disease.
- Prompt pelvic ultrasound and/or pelvic MRI; use O-RADS risk stratification and gynecologic referral when appropriate.
- Hemorrhagic-appearing cyst after menopause usually needs US or MRI characterization.