Incidental Adrenal Lesions
Quick Reference Images
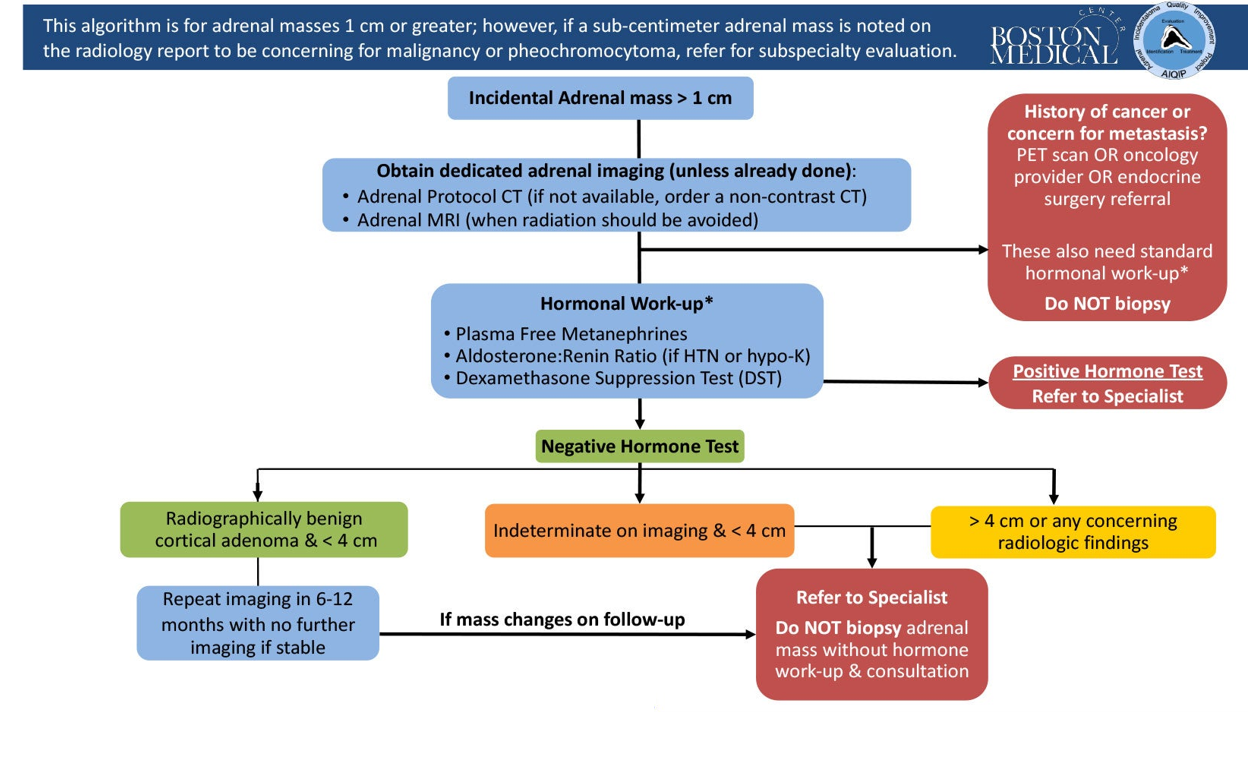
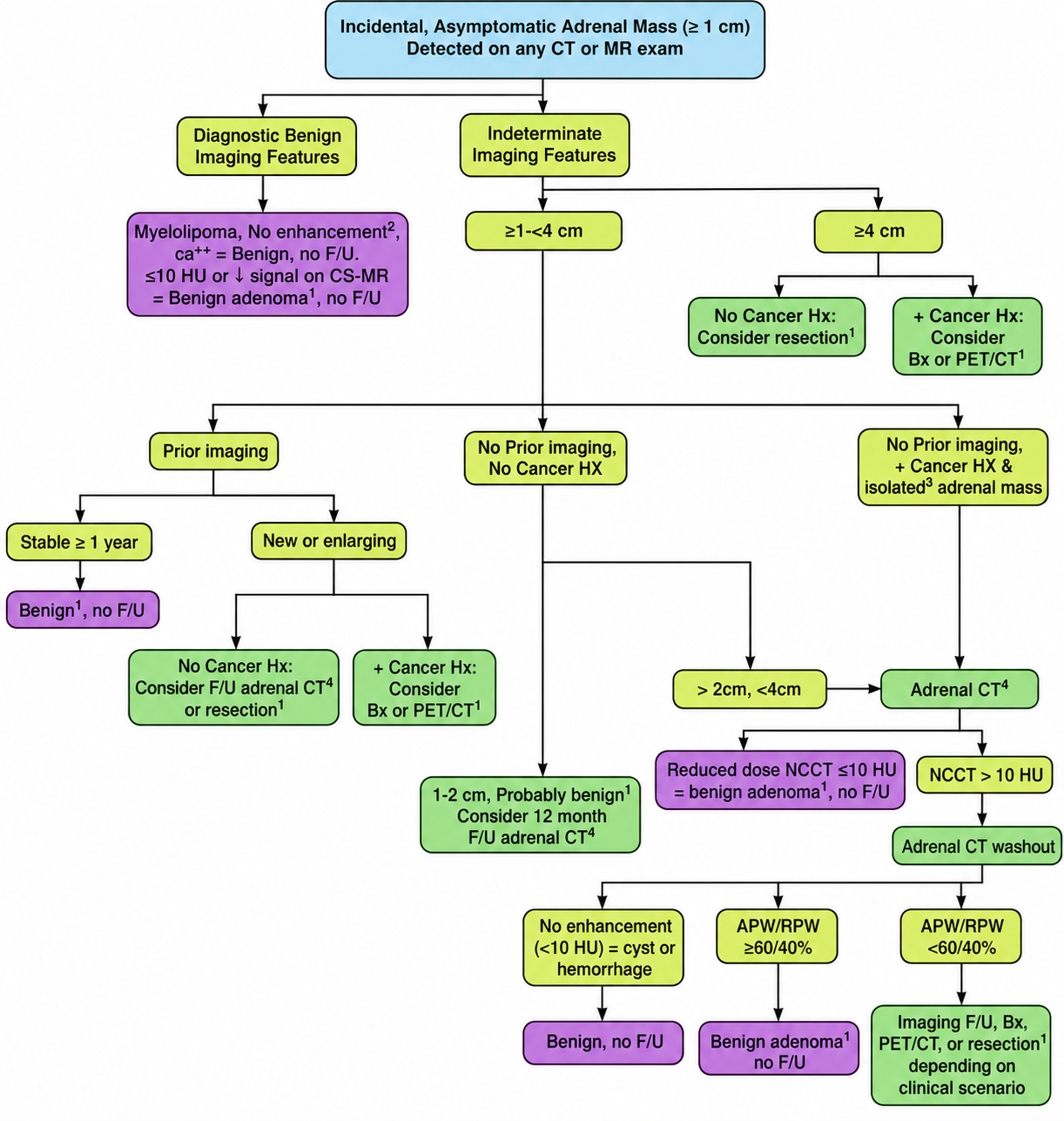
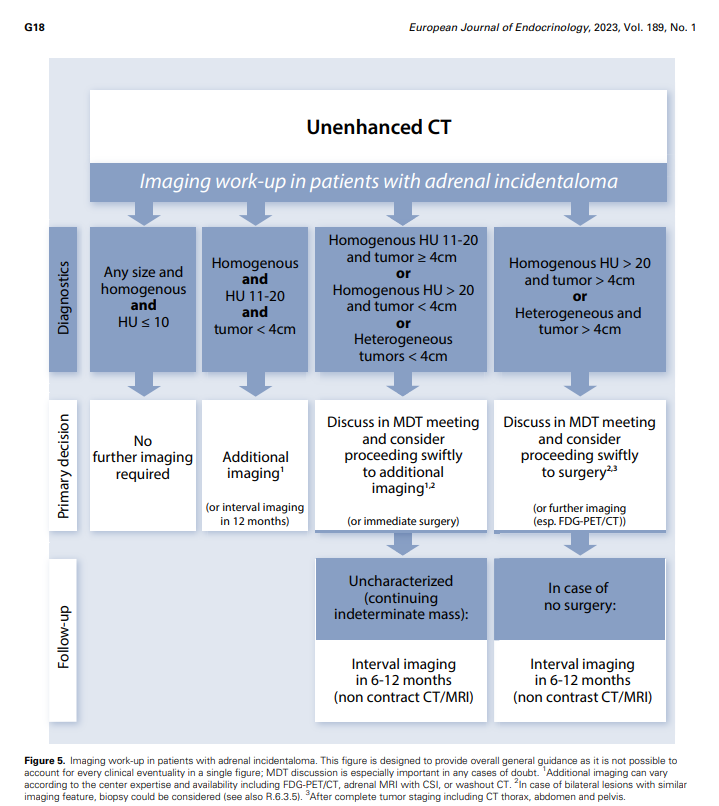
Imaging Algorithm
< 1 cm
Usually no imaging workup in adults unless there is a suspicious clinical context.
Clearly benign - no follow-up
- Homogeneous adrenal lesion with noncontrast CT density <= 10 HU.
- Macroscopic fat: classic myelolipoma.
- Clear signal drop on chemical-shift MRI, consistent with lipid-rich adenoma.
- Simple cyst, chronic hemorrhage, or benign calcified lesion with stable benign appearance.
- Modern guidance does not require a size cutoff when benign adenoma imaging criteria are fulfilled.
1-4 cm indeterminate lesion
- Check prior imaging first. Stability for at least 1 year strongly favors benignity.
- If homogeneous, HU 11-20, and < 4 cm: consider immediate additional characterization or interval CT/MRI in 12 months.
- If < 4 cm but HU > 20 or heterogeneous: discuss / characterize with adrenal protocol CT or MRI.
- If known extra-adrenal malignancy: consider adrenal protocol CT, FDG-PET/CT, biopsy, or surgery based on staging impact.
>= 4 cm or suspicious
- Heterogeneous lesion or HU > 20: multidisciplinary review; surgery is often favored in fit patients.
- If surgery is not performed, repeat noncontrast CT or MRI in 6-12 months.
Adrenal CT / MRI
Adrenal protocol CT
- Use when noncontrast CT density is > 10 HU and morphology is not definitively benign.
- Typical protocol: noncontrast, enhanced venous/equilibrium, and delayed images.
- Adenoma washout: absolute washout >= 60% or relative washout >= 40%.
- Discordant washout, growth, heterogeneity, or suspicious clinical context should remain indeterminate.
Chemical-shift MRI
- Useful when CT is indeterminate or when radiation avoidance is preferred.
- Signal drop on opposed-phase images supports intracellular lipid and lipid-rich adenoma.
- Lack of signal drop does not exclude adenoma; lipid-poor adenoma remains possible.
When still indeterminate
- Compare with prior imaging whenever available.
- Use growth, heterogeneity, HU, washout, and cancer history to decide follow-up versus referral.
- Biopsy is generally reserved for selected patients with known extra-adrenal malignancy when the result will change management.
Refer, Follow, Or Stop
Stop imaging follow-up
Homogeneous HU <= 10 lesion, classic lipid-rich adenoma, myelolipoma, or other unequivocally benign lesion.
Refer / surgery
- Indeterminate mass > 4 cm, heterogeneous, irregular, HU > 20, or enlarging.
- Younger patients, pregnant patients, and patients with concerning imaging should be discussed early with a multidisciplinary team.
Follow-up if not resected
- Indeterminate lesion: repeat noncontrast CT or MRI at 6-12 months.
- Concerning growth: > 20% increase in maximum diameter plus at least 5 mm absolute growth favors resection.
- If growth is below threshold, another 6-12 month follow-up may be considered.