Fleischner 2017 Pulmonary Nodule Guidelines
Reference Images
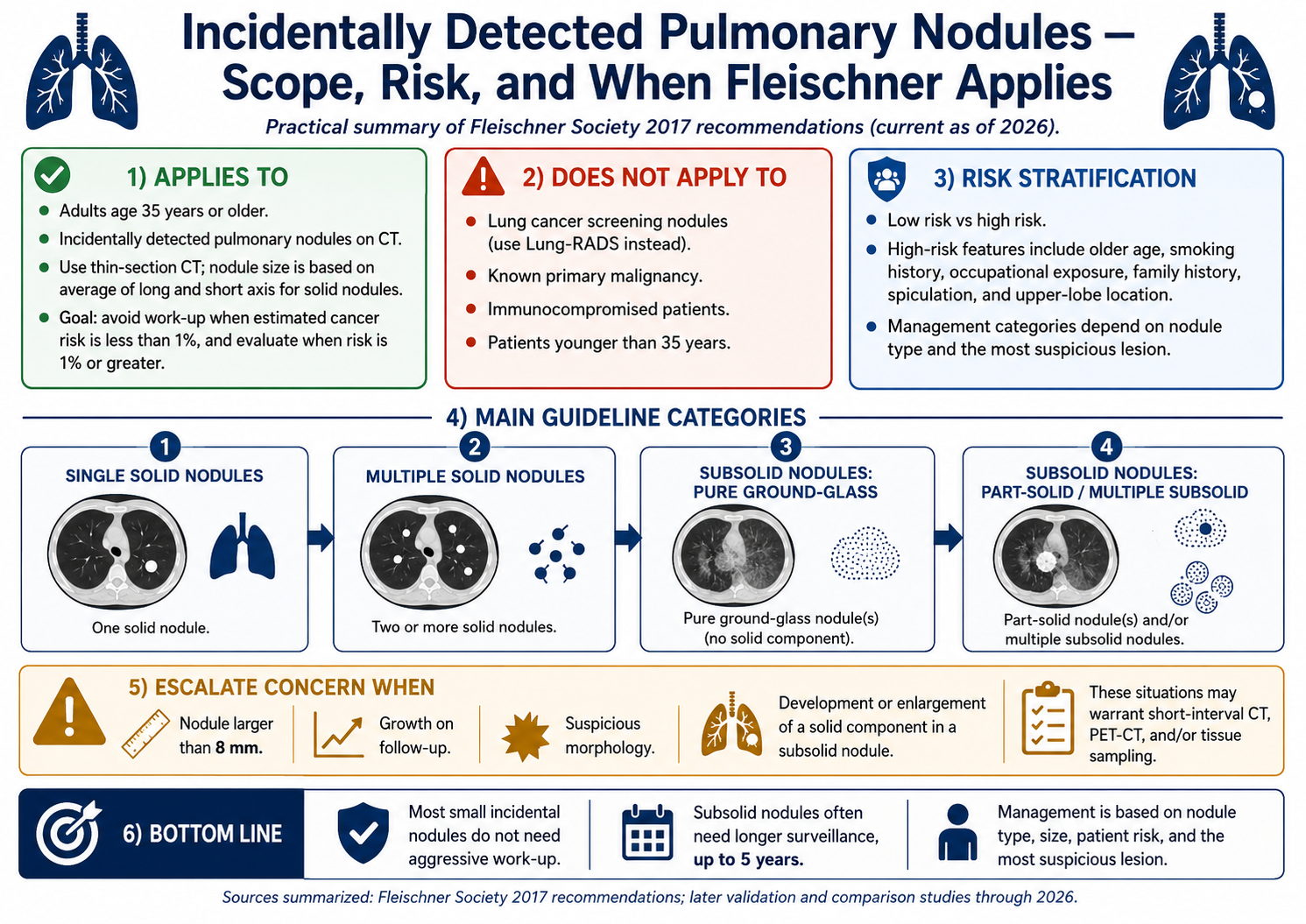
Scope / Risk
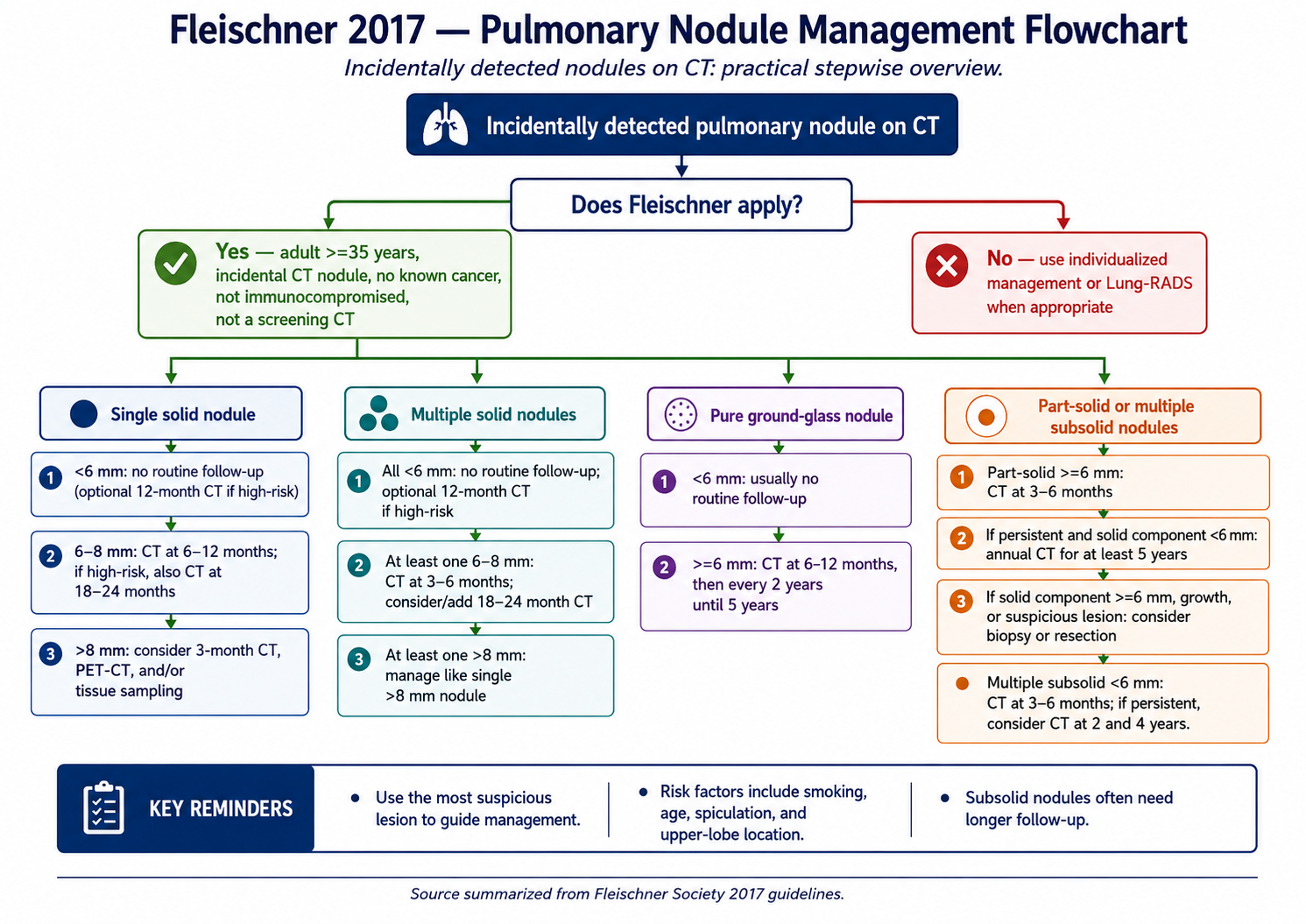
Use Fleischner when
Adult 35 years or older with an incidentally detected pulmonary nodule on CT.
Does not apply
- Lung cancer screening nodules: use Lung-RADS.
- Known primary malignancy, immunocompromised patients, or patients younger than 35 years.
- Management is individualized when Fleischner does not apply.
Risk features
- High-risk features include older age, smoking history, occupational exposure, family history, spiculation, and upper-lobe location.
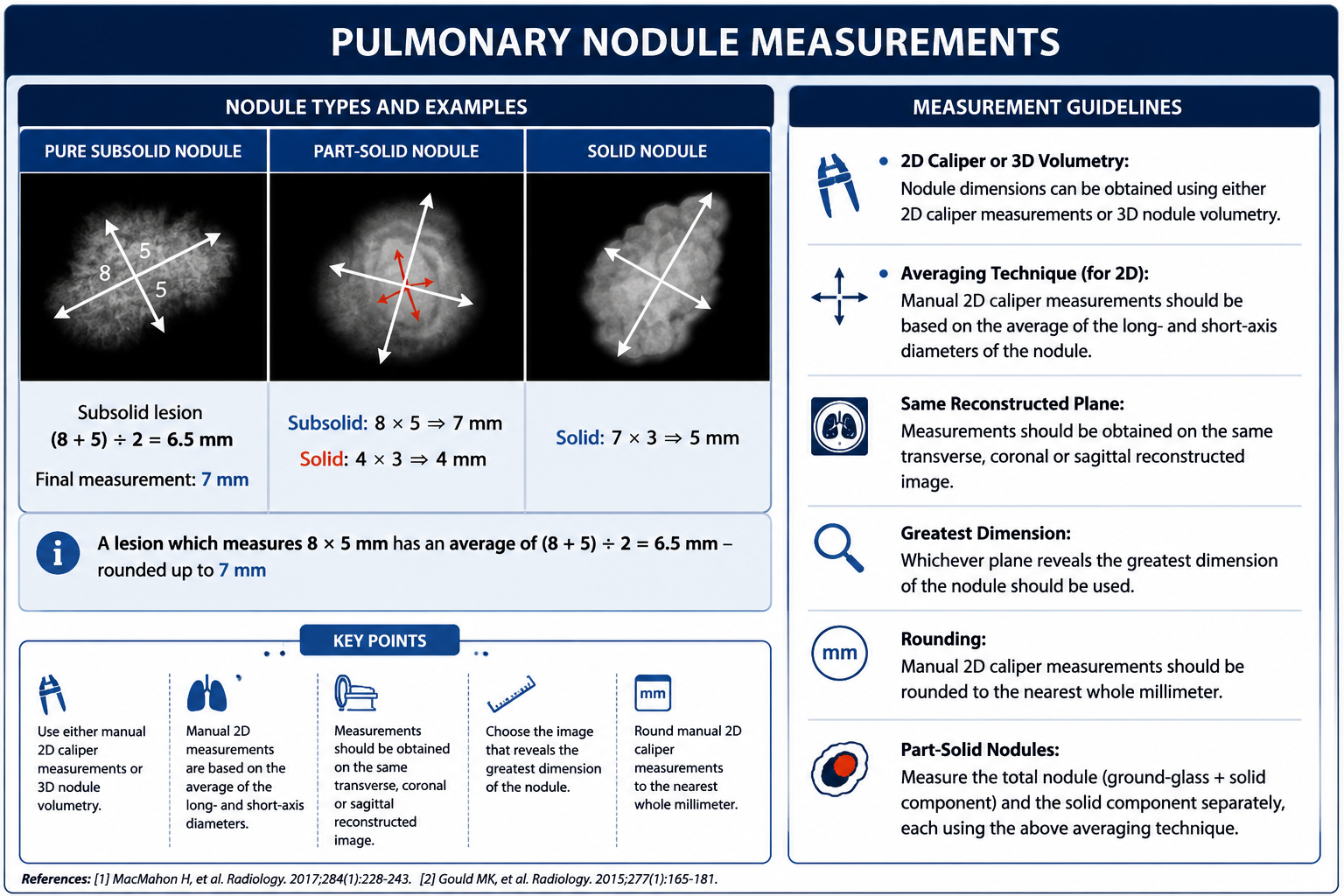
- Use thin-section CT and base solid nodule size on the average of long and short axes.
- Use the most suspicious nodule to guide management when multiple nodules are present.
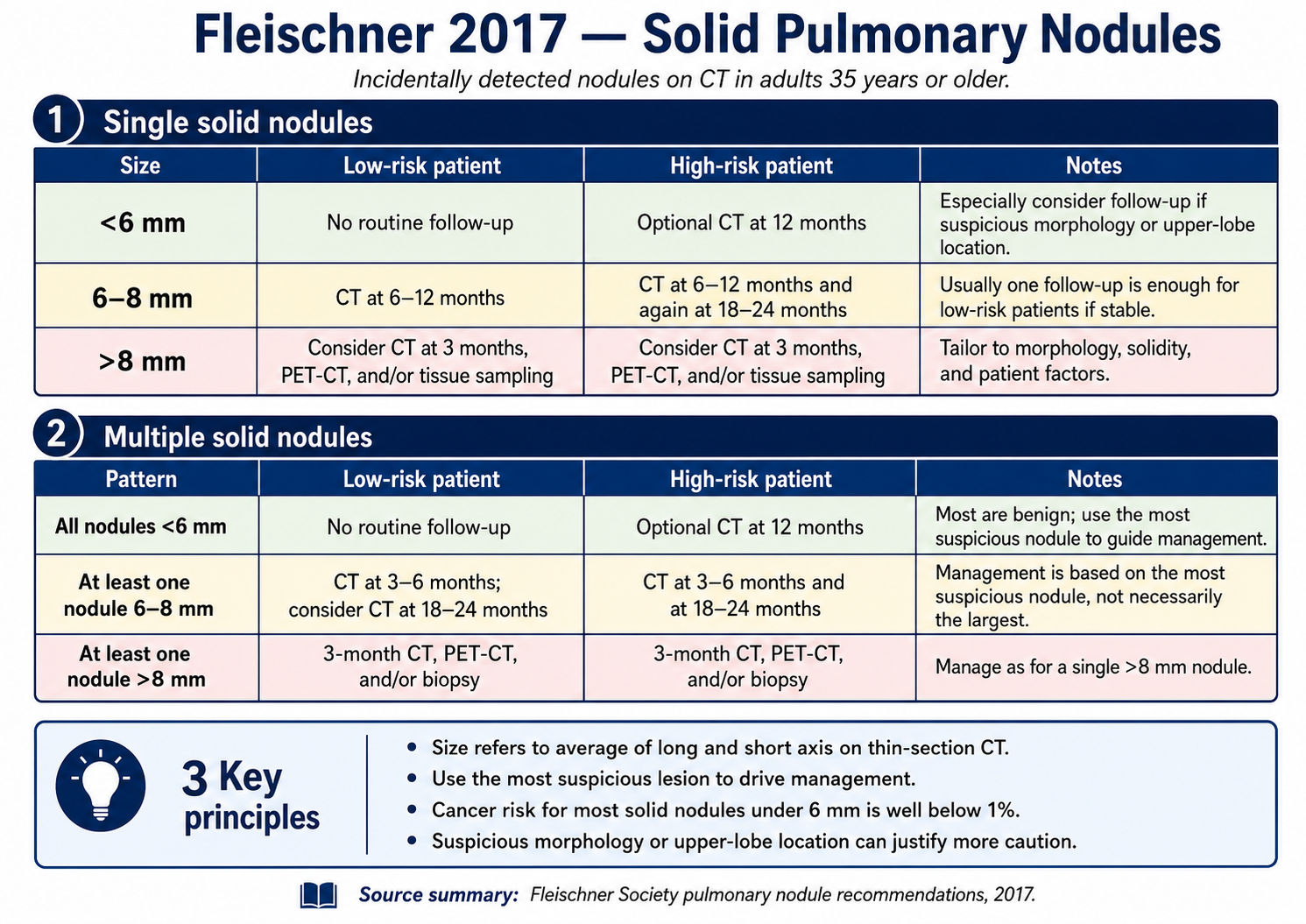
Solid Nodules
Single solid nodule
- Less than 6 mm: low risk no routine follow-up; high risk optional CT at 12 months.
- 6-8 mm: low risk CT at 6-12 months; high risk CT at 6-12 months and again at 18-24 months.
- Greater than 8 mm: consider CT at 3 months, PET-CT, and/or tissue sampling.
Multiple solid nodules
- All less than 6 mm: low risk no routine follow-up; high risk optional CT at 12 months.
- At least one 6-8 mm: CT at 3-6 months; high risk also CT at 18-24 months.
- At least one greater than 8 mm: manage like a single greater than 8 mm nodule.
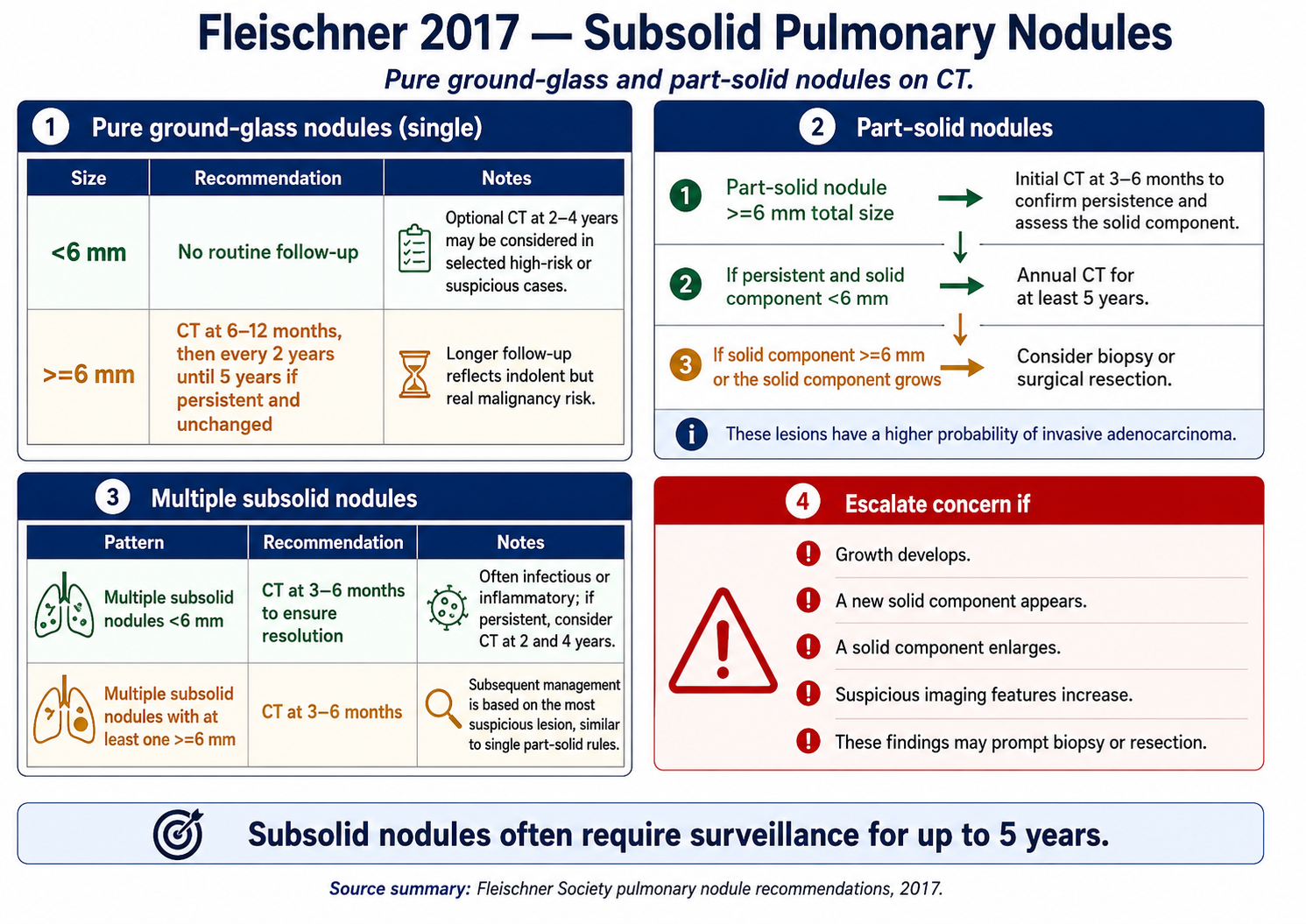
Subsolid / Special
Pure ground-glass nodules
- Less than 6 mm: generally no routine follow-up; optional CT at 2-4 years in selected high-risk or suspicious cases.
- 6 mm or larger: CT at 6-12 months, then every 2 years until 5 years if persistent and unchanged.
Part-solid / multiple subsolid
- Part-solid 6 mm or larger: CT at 3-6 months to confirm persistence and assess the solid component.
- If persistent with solid component less than 6 mm: annual CT for at least 5 years.
- Solid component 6 mm or larger, growth, or suspicious morphology: consider biopsy or surgical resection.
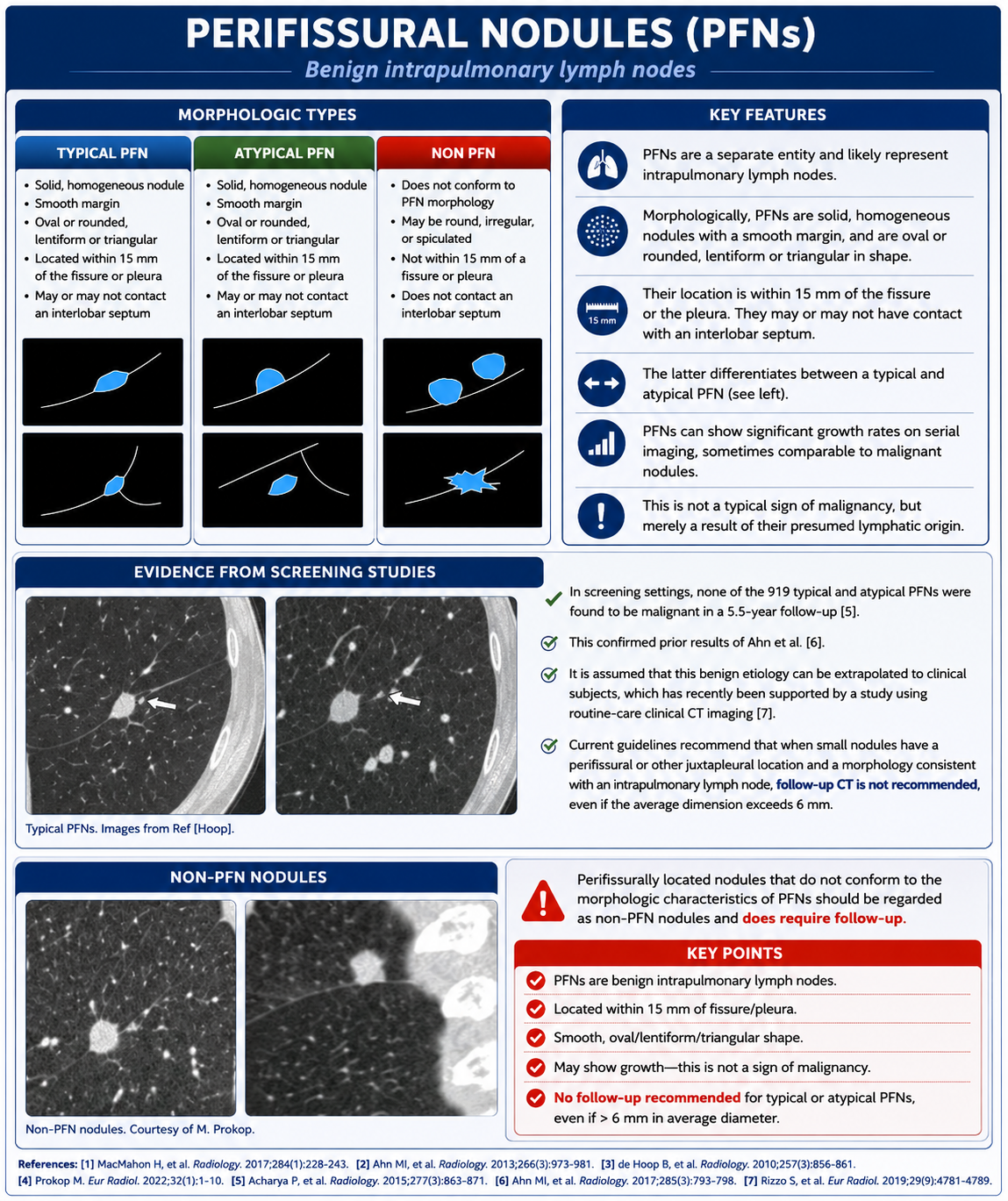
- Typical perifissural nodules do not need follow-up when morphology is consistent with intrapulmonary lymph node.