Incidental Gallbladder and Biliary Findings
Reference Images
Initial Triage
First question
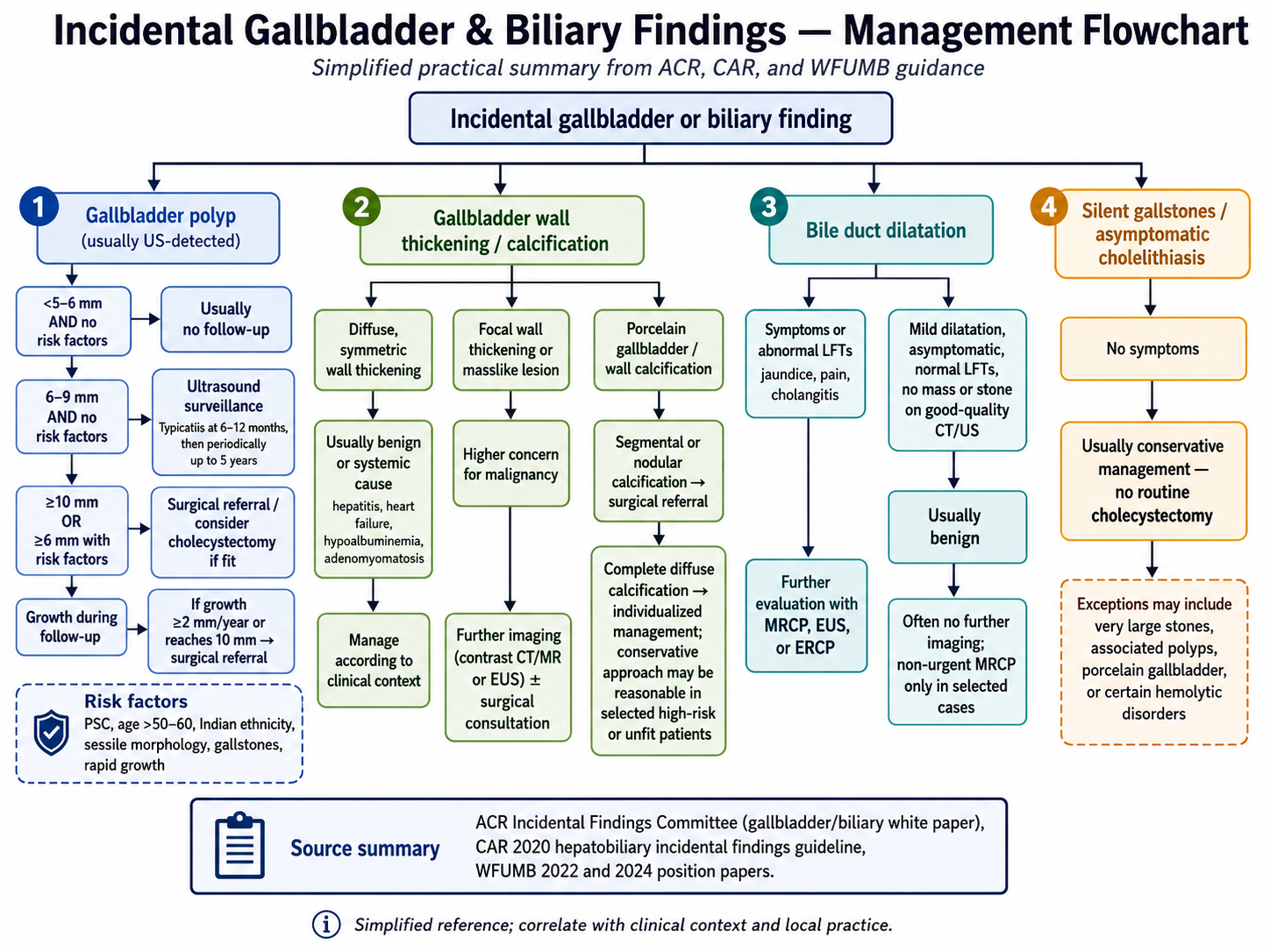
Separate gallbladder polyp, wall abnormality, bile duct dilatation, and silent gallstones before choosing the pathway.
Gallbladder polyps
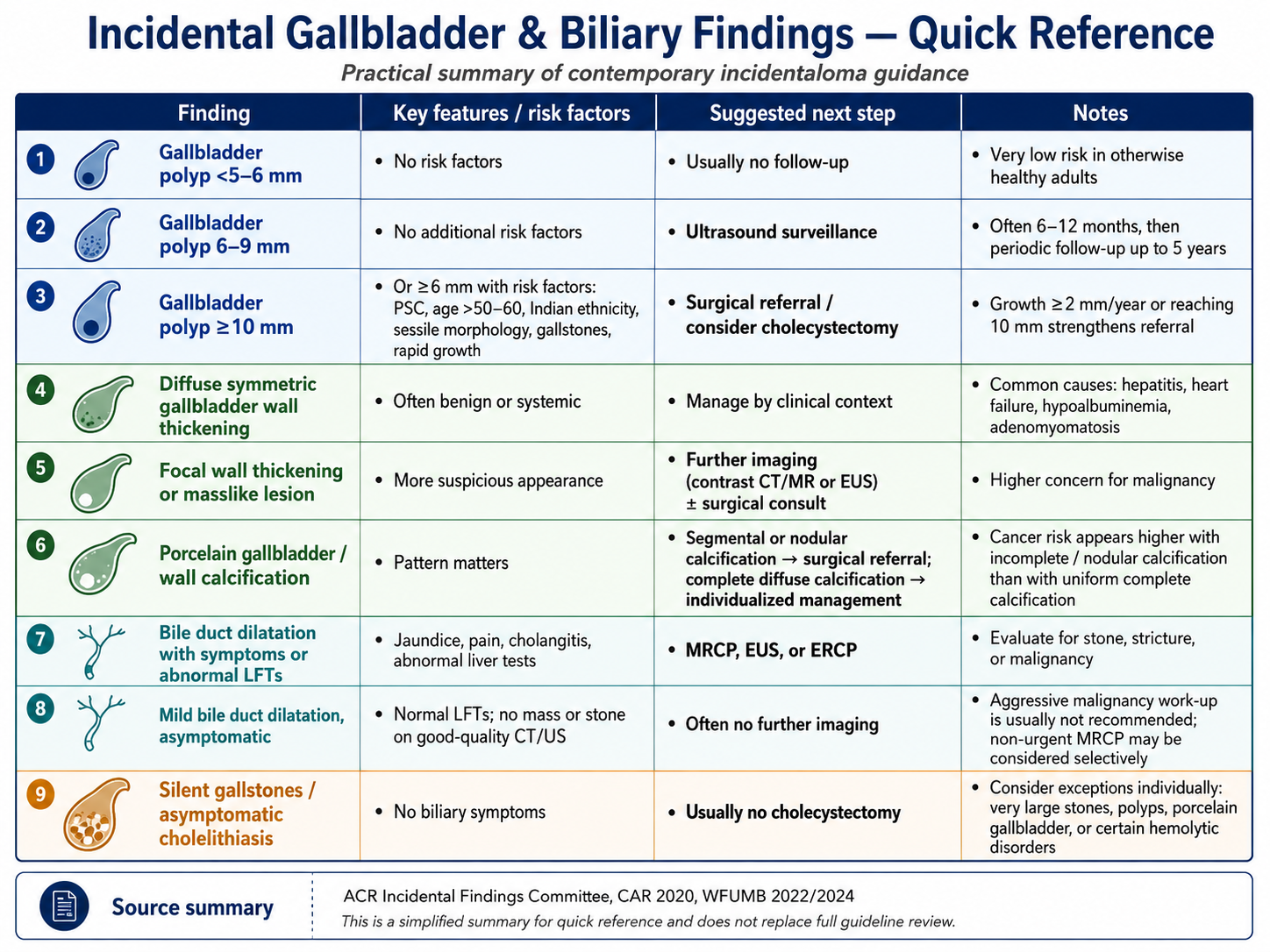
- Less than 5-6 mm and no risk factors: usually no follow-up.
- 6-9 mm without additional risk factors: ultrasound surveillance, often starting at 6-12 months.
- 10 mm or larger, or 6 mm or larger with risk factors: surgical referral or consider cholecystectomy if fit.
Risk factors
- PSC, age over 50-60, Indian ethnicity, sessile morphology, gallstones, or rapid growth.
- Growth by 2 mm/year or reaching 10 mm strengthens surgical referral.
Wall / Calcification
Wall thickening
- Diffuse symmetric wall thickening is often benign or systemic: hepatitis, heart failure, hypoalbuminemia, or adenomyomatosis.
- Manage diffuse symmetric thickening according to clinical context.
- Focal wall thickening or masslike lesion is higher concern for malignancy.
Porcelain gallbladder
- Segmental or nodular calcification has higher concern and generally warrants surgical referral.
- Complete diffuse calcification may be individualized, especially in high-risk or unfit patients.
- Focal suspicious wall findings: contrast CT/MR or EUS with surgical consultation.
Ducts / Stones
Bile duct dilatation
- Symptoms, jaundice, cholangitis, pain, or abnormal LFTs: evaluate with MRCP, EUS, or ERCP.
- Mild dilatation with normal LFTs and no mass or stone on good-quality CT/US is usually benign.
- Non-urgent MRCP can be considered selectively when uncertainty remains.
Silent gallstones
- Asymptomatic cholelithiasis usually gets conservative management, not routine cholecystectomy.
- Possible exceptions: very large stones, associated polyps, porcelain gallbladder, or selected hemolytic disorders.