Incidental Liver Lesions
Quick Reference Images
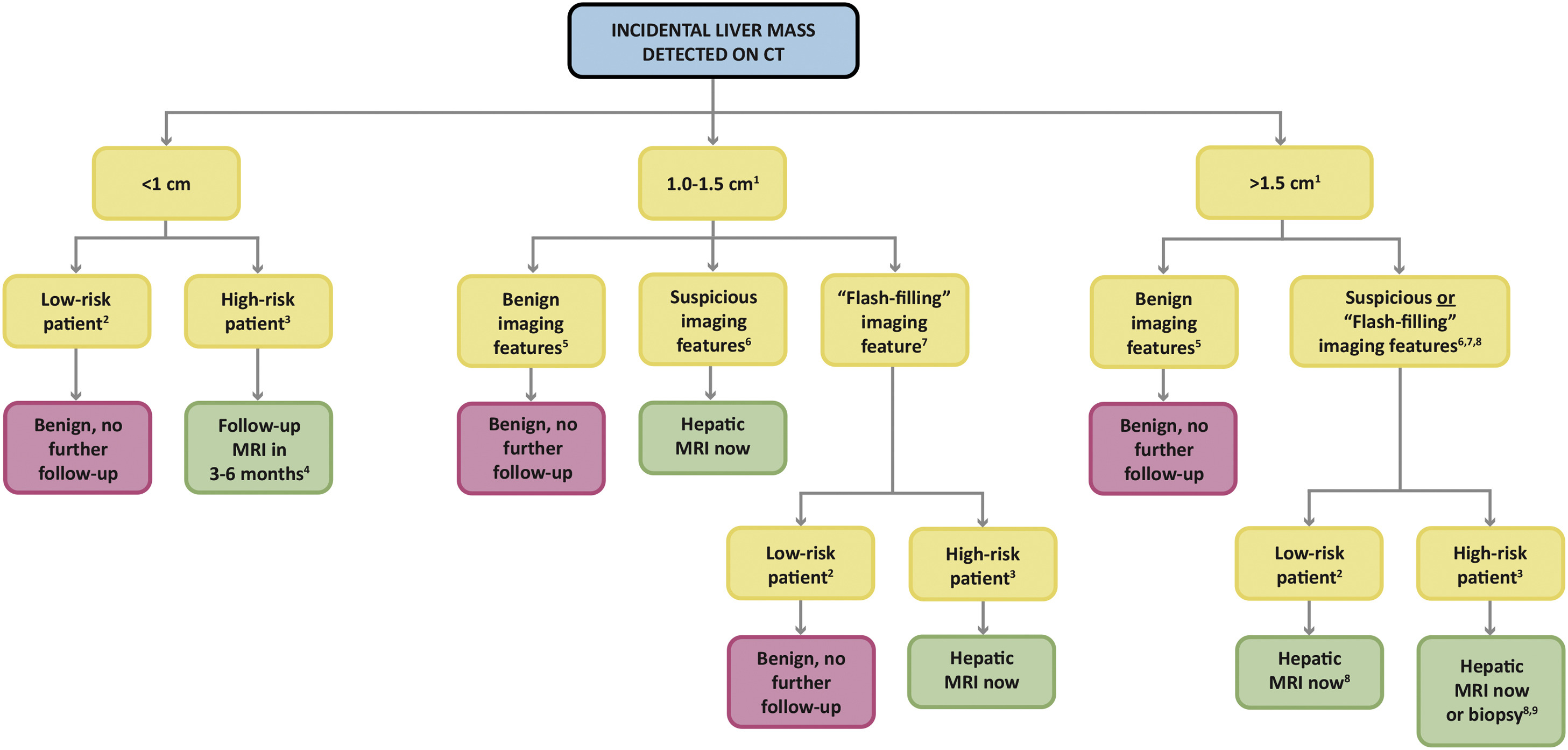
Initial Triage
First question
Known malignancy, cirrhosis, chronic hepatitis, or other HCC risk changes the pathway.
No cancer / no HCC risk
- Many incidental lesions are benign: cyst, hemangioma, FNH, focal fat, or perfusional change.
- Subcentimeter lesion with benign features usually needs no follow-up.
- Indeterminate lesion on ultrasound or single-phase CT: characterize with contrast MRI or multiphasic CT.
Cancer or chronic liver disease
- Lower threshold for dedicated multiphasic CT/MRI.
- Cirrhotic or HCC-risk patients should generally use LI-RADS rather than this page.
- Known cancer history: evaluate for metastasis if imaging features are not diagnostic benign.
Benign Patterns
No follow-up when classic
- Simple cyst: water attenuation/signal, no enhancement, no solid component.
- Hemangioma: peripheral nodular discontinuous enhancement with progressive fill-in.
- FNH: arterial hyperenhancement, central scar when present, and typical hepatobiliary phase retention.
- Focal fat or focal fat sparing in characteristic locations with no mass effect.
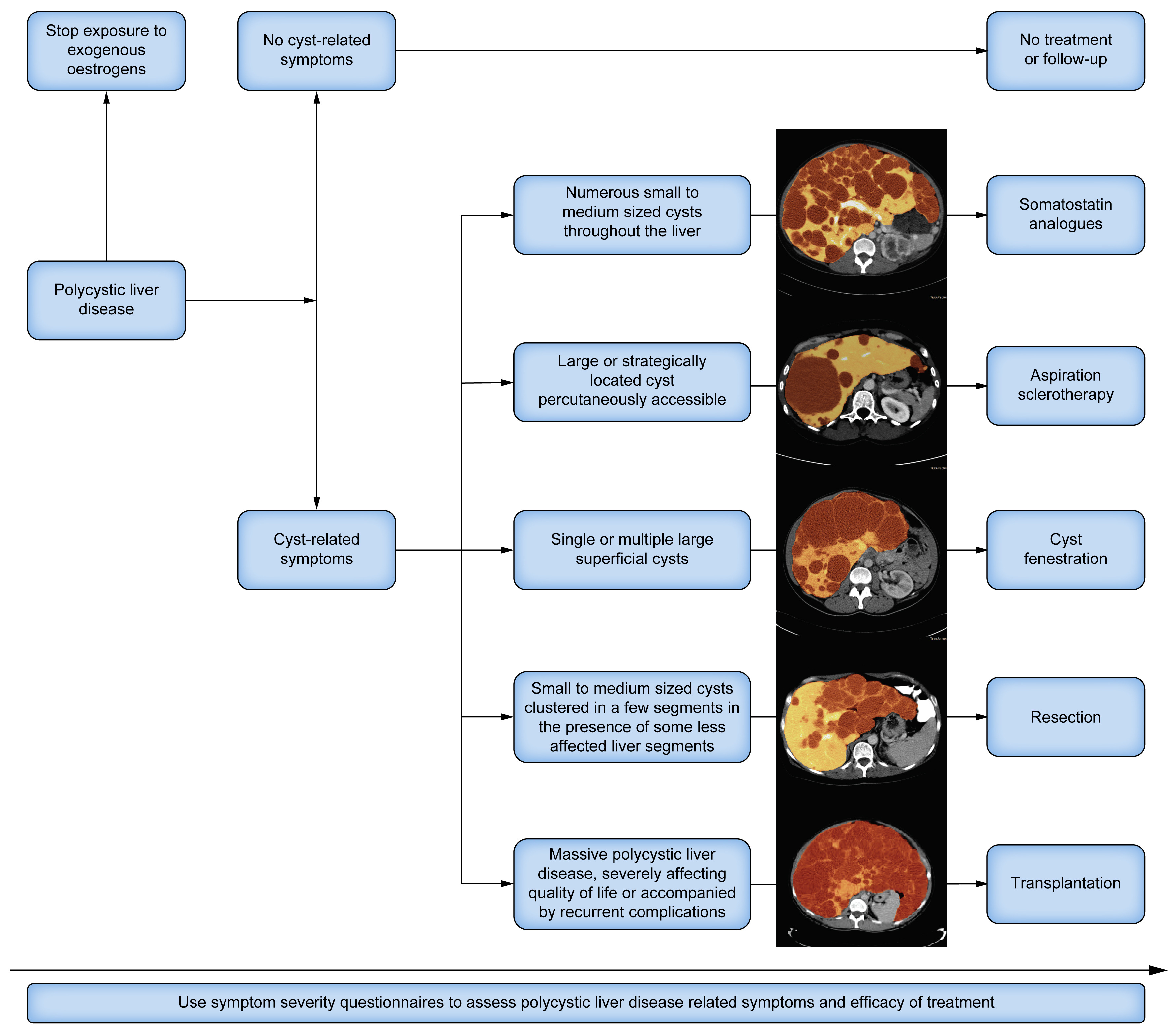
Polycystic liver disease
- No cyst-related symptoms: usually no treatment or follow-up.
- Symptomatic dominant cyst: aspiration/sclerotherapy or fenestration may be considered.
- Diffuse severe symptomatic disease: specialty referral for medical, surgical, or transplant options.
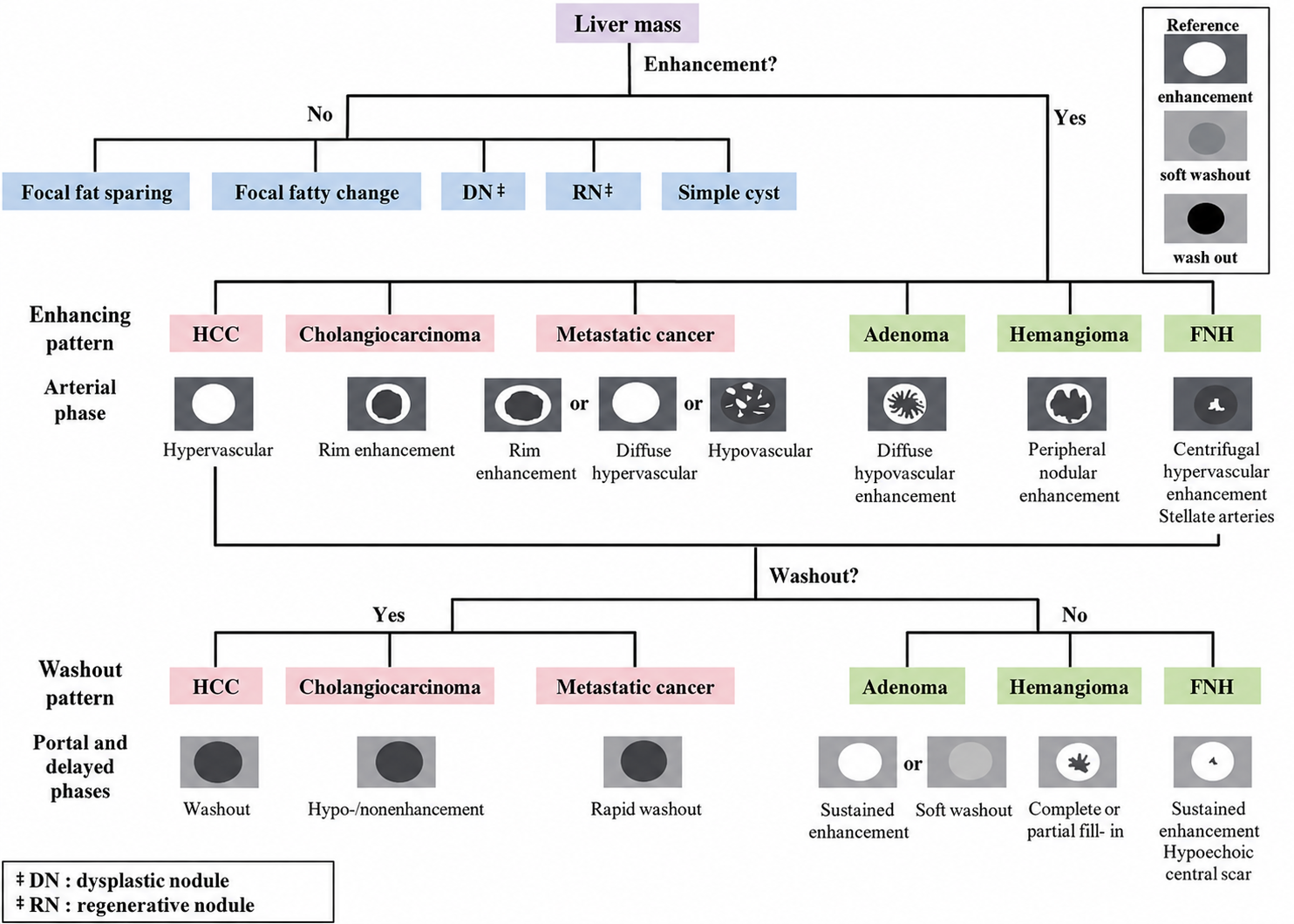
Indeterminate / Suspicious
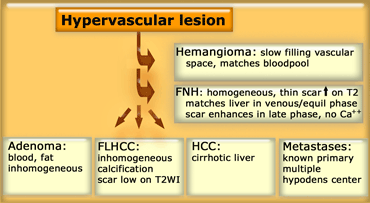
Hypervascular lesion
- Benign possibilities: hemangioma, FNH, adenoma, perfusional phenomenon.
- Suspicious possibilities: HCC in at-risk liver, hypervascular metastasis, cholangiocarcinoma, or mixed tumor.
- Use arterial, portal venous, delayed, and hepatobiliary phase patterns when available.
Adenoma / suspicious mass
- Hepatic adenoma management depends on size, subtype, growth, sex, and hormone exposure.
- Lesions around 5 cm or larger, growing, hemorrhagic, or beta-catenin subtype often need specialty management.
- If still indeterminate after high-quality imaging, consider short interval follow-up, multidisciplinary review, or biopsy.