Lung-RADS v2022
Reference Images
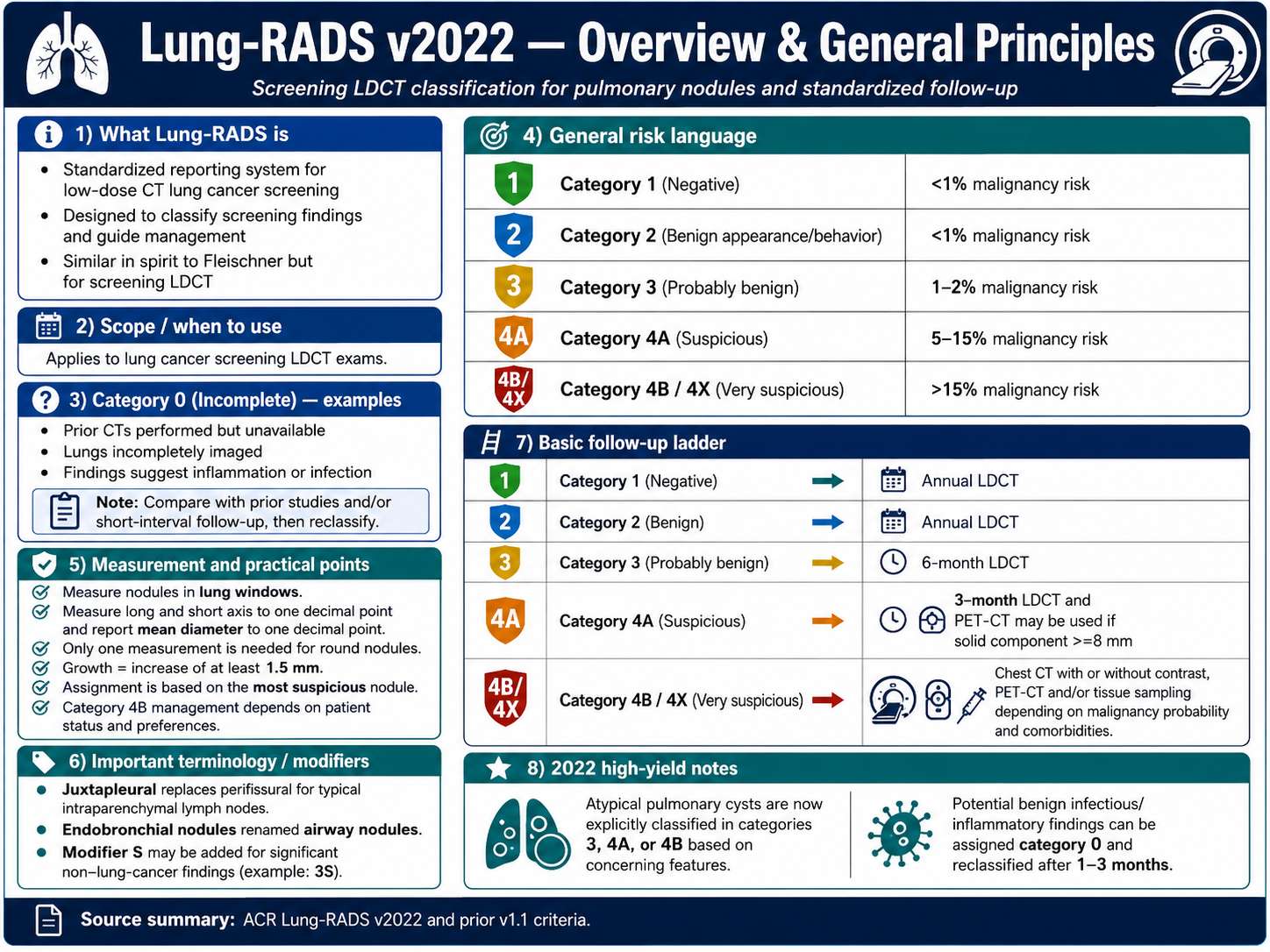
Overview
Use Lung-RADS when
Low-dose CT lung cancer screening exam. Use Fleischner or individualized management for incidental diagnostic CT nodules.
General principles
- Category assignment is based on the most suspicious nodule.
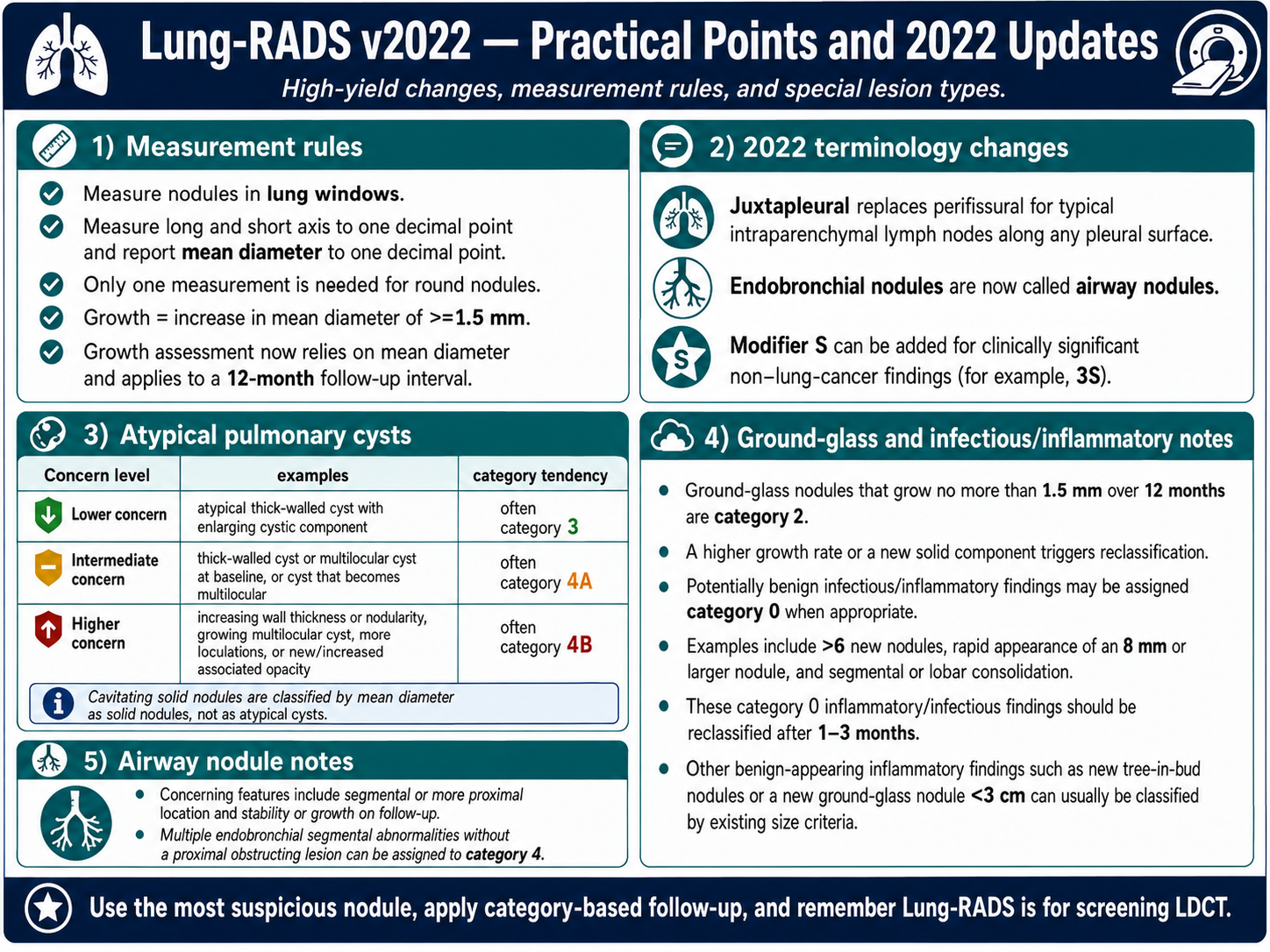
- Measure in lung windows; report mean diameter to one decimal point.
- Growth is an increase in mean diameter of at least 1.5 mm.
- Use modifier S for clinically significant non-lung-cancer findings when appropriate.
Basic follow-up ladder
- Categories 1 and 2: annual LDCT.
- Category 3: 6-month LDCT.
- Category 4A: 3-month LDCT; PET-CT may be useful when solid component is at least 8 mm.
- Categories 4B and 4X: diagnostic chest CT, PET-CT, and/or tissue sampling depending on context.
Categories 0-4A
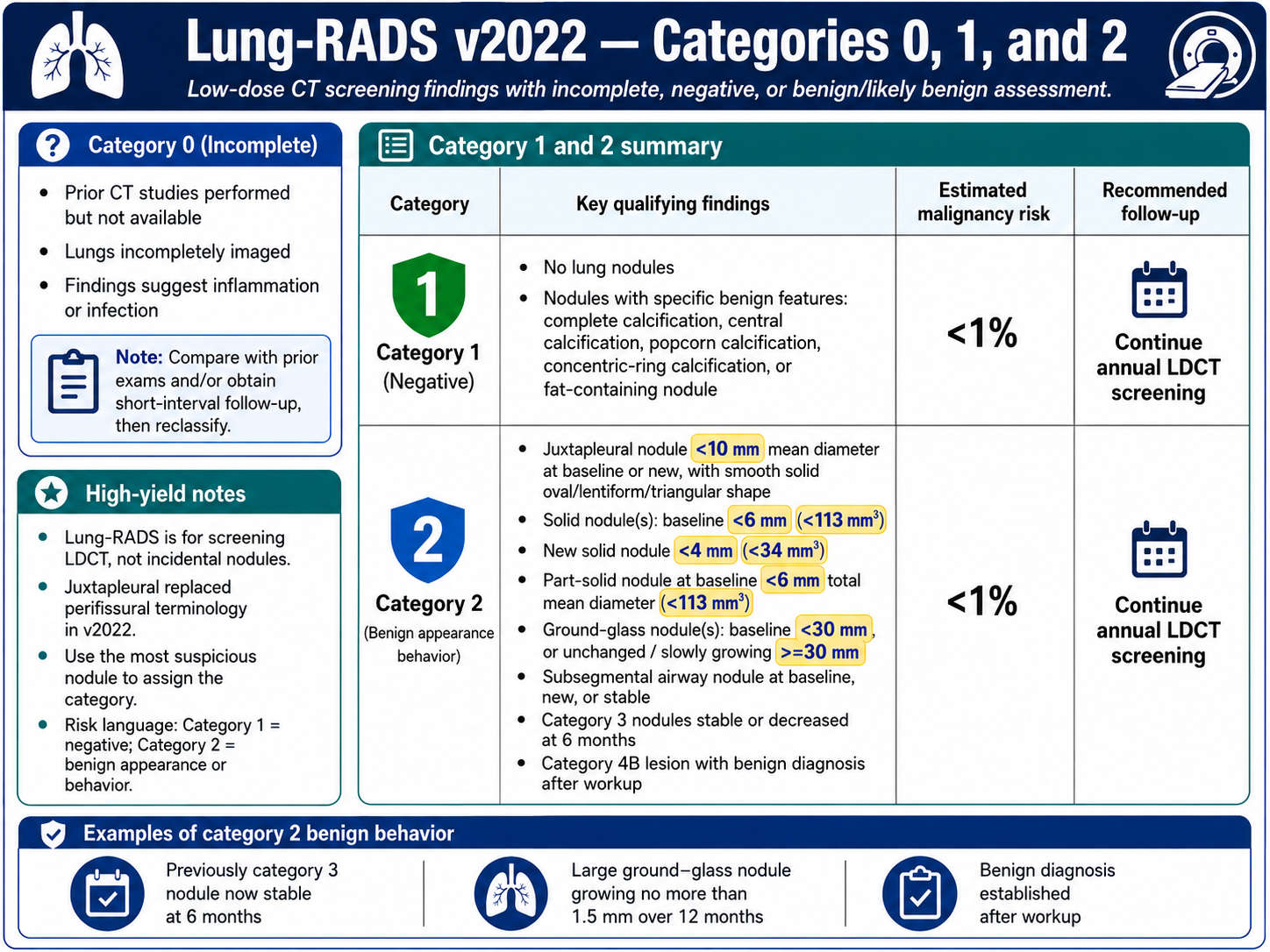
0, 1, and 2
- Category 0: incomplete exam or findings needing comparison, additional imaging, or short-interval reassessment.
- Category 1: negative; annual LDCT.
- Category 2: benign appearance or behavior; annual LDCT.
- Juxtapleural nodules with benign morphology can be category 2 in v2022.
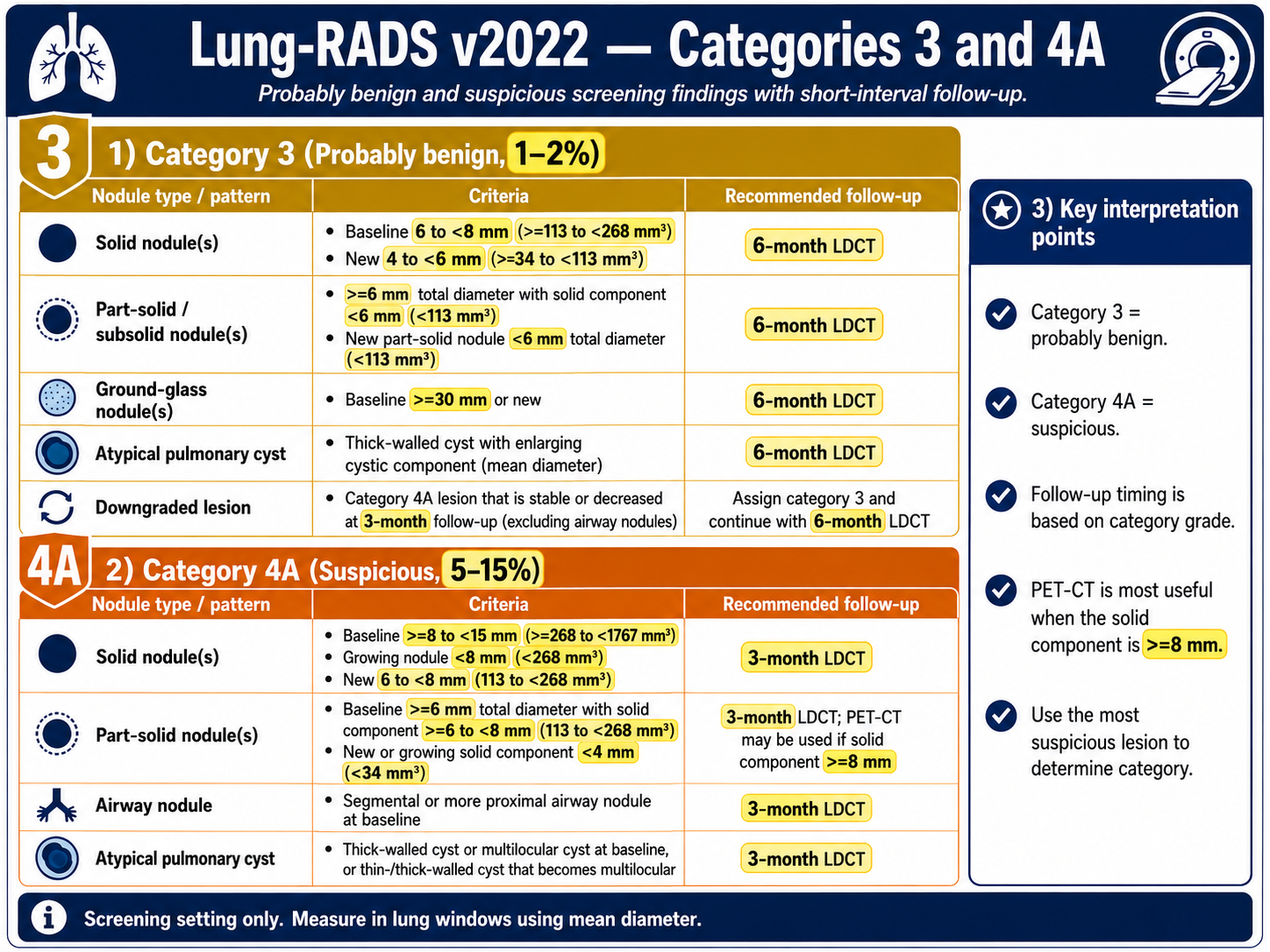
3 and 4A
- Category 3: probably benign, estimated 1-2% malignancy risk; 6-month LDCT.
- Category 4A: suspicious, estimated 5-15% malignancy risk; 3-month LDCT.
- Category 4A lesions that are stable or decreased at 3-month follow-up can be assigned category 3 with 6-month LDCT.
- PET-CT is most useful when the solid component is at least 8 mm.
4B / 4X / Updates
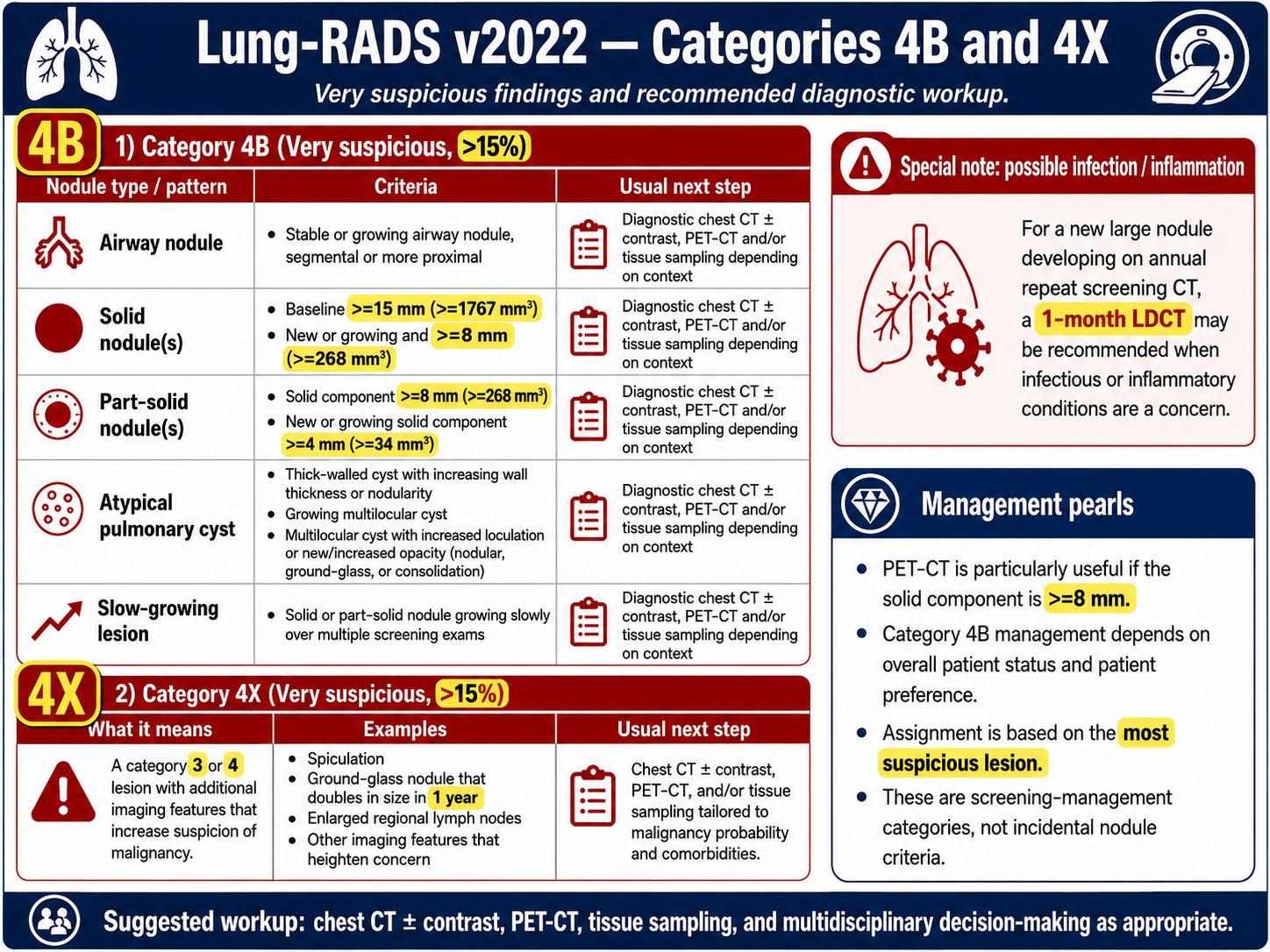
Very suspicious categories
- Category 4B: very suspicious, estimated greater than 15% malignancy risk.
- Category 4X: category 3 or 4 lesion with additional imaging features that increase suspicion.
- Usual workup: diagnostic chest CT with or without contrast, PET-CT, and/or tissue sampling.
- If a new large nodule may be infectious or inflammatory, 1-month LDCT may be appropriate.
v2022 high-yield updates
- Juxtapleural replaces perifissural terminology for typical intraparenchymal lymph nodes along pleural surfaces.
- Endobronchial nodules are now called airway nodules.
- Atypical pulmonary cysts are explicitly classified as category 3, 4A, or 4B based on concerning features.
- Potential infectious or inflammatory findings may be assigned category 0 and reclassified after 1-3 months.