Incidental Pancreatic Cystic Lesions
Quick Reference Flowcharts
Initial Imaging
< 5 mm
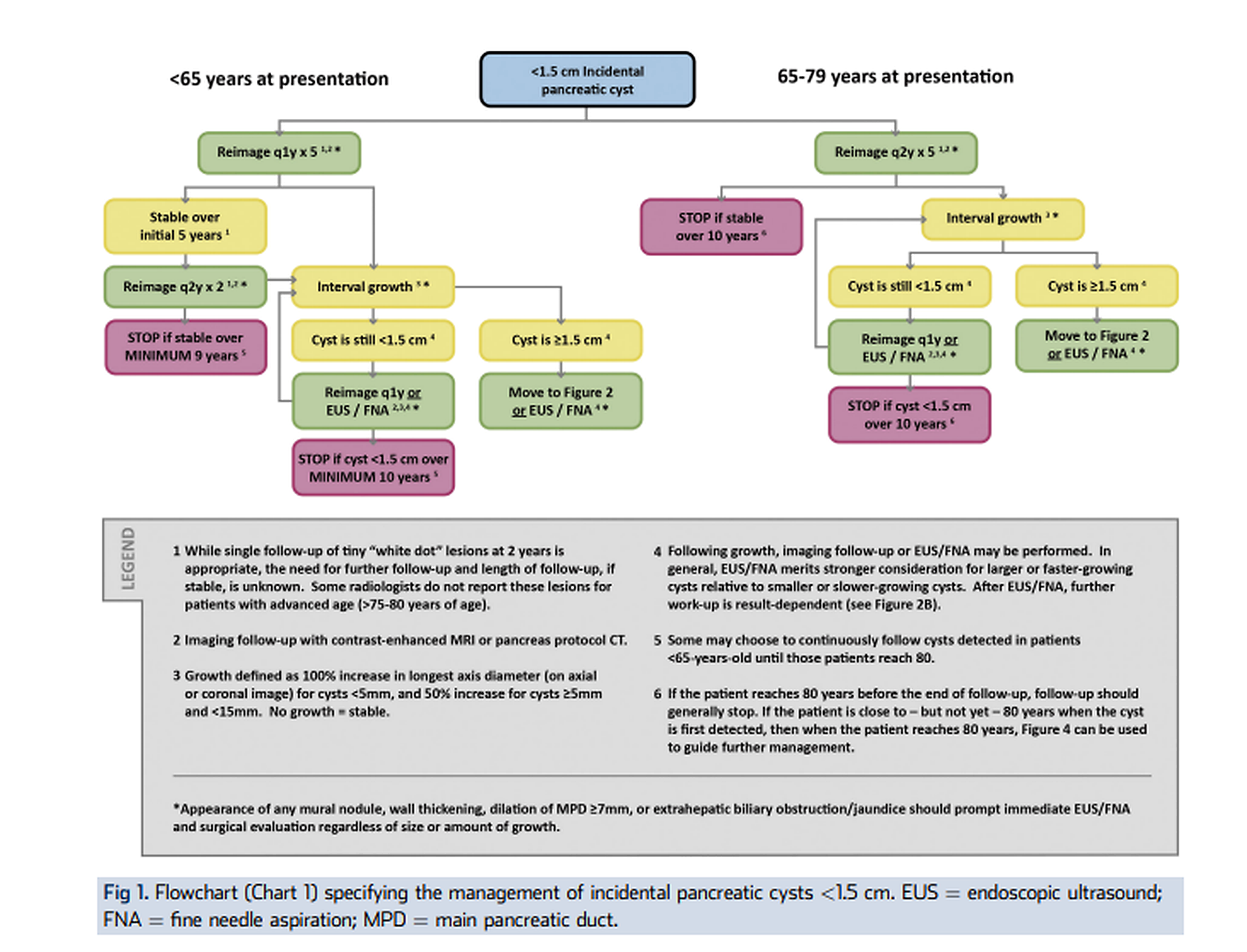
Very small asymptomatic cysts are usually low risk. A single CT or MRI at about 2 years can document stability in patients younger than 75; follow-up is often unnecessary in older patients.
Preferred characterization
- MRI with MRCP is usually preferred for duct communication, septations, mural nodules, and main pancreatic duct anatomy.
- Pancreatic protocol contrast CT is acceptable when MRI is contraindicated or unavailable.
- Report cyst size, location, duct communication if visible, MPD caliber, wall thickening/enhancement, mural nodule, solid component, and interval growth.
Likely benign entities
- Serous cystadenoma: classic microcystic honeycomb appearance, with or without central scar; often no long-term surveillance once confidently diagnosed.
- Pseudocyst: appropriate pancreatitis history and typical appearance; does not need oncologic-type cyst surveillance once resolved.
- Mucinous cysts, branch-duct IPMN, main-duct IPMN, and MCN carry malignant potential and drive surveillance decisions.
Risk Features
Worrisome features
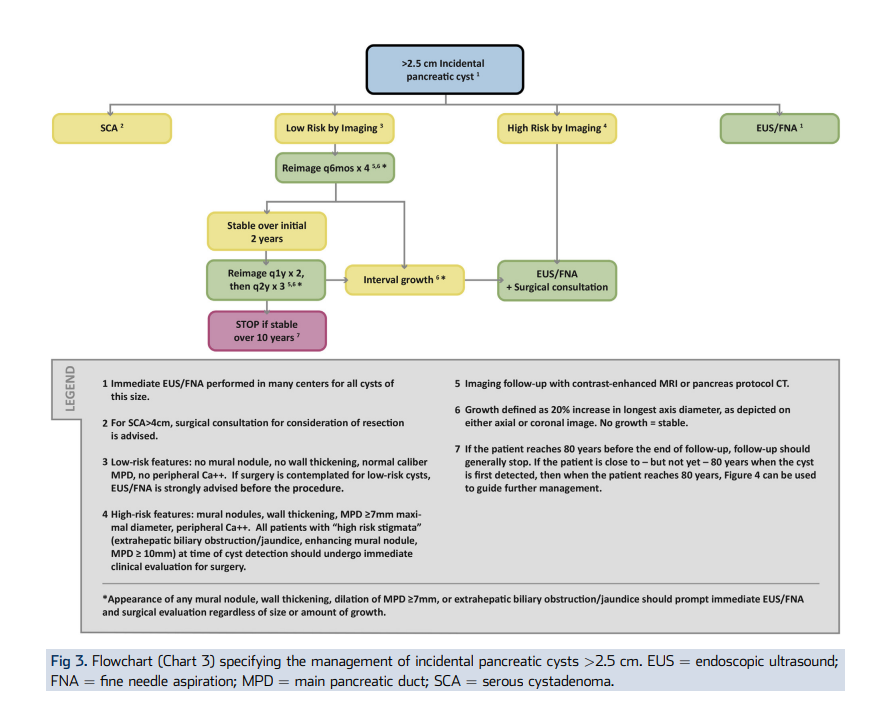
- Cyst size >= 3 cm.
- Thickened or enhancing cyst wall.
- Non-enhancing mural nodule or small solid component.
- Main pancreatic duct about 5-9 mm.
- Abrupt duct caliber change with distal pancreatic atrophy.
- Documented growth, especially about >= 2.5 mm/year.
High-risk stigmata
- Obstructive jaundice with a cystic lesion in the pancreatic head.
- Enhancing mural nodule or solid component >= 5 mm.
- Main pancreatic duct >= 10 mm.
- Suspicious or positive cytology, when available.
Escalate
Any high-risk feature or multiple worrisome features should prompt EUS +/- FNA and multidisciplinary review if the patient is a treatment candidate.
Surveillance / Escalation
No worrisome features
- 5 mm to < 2 cm: MRI or CT at roughly 1-2 year intervals initially; extend or stop after prolonged stability depending on age and guideline preference.
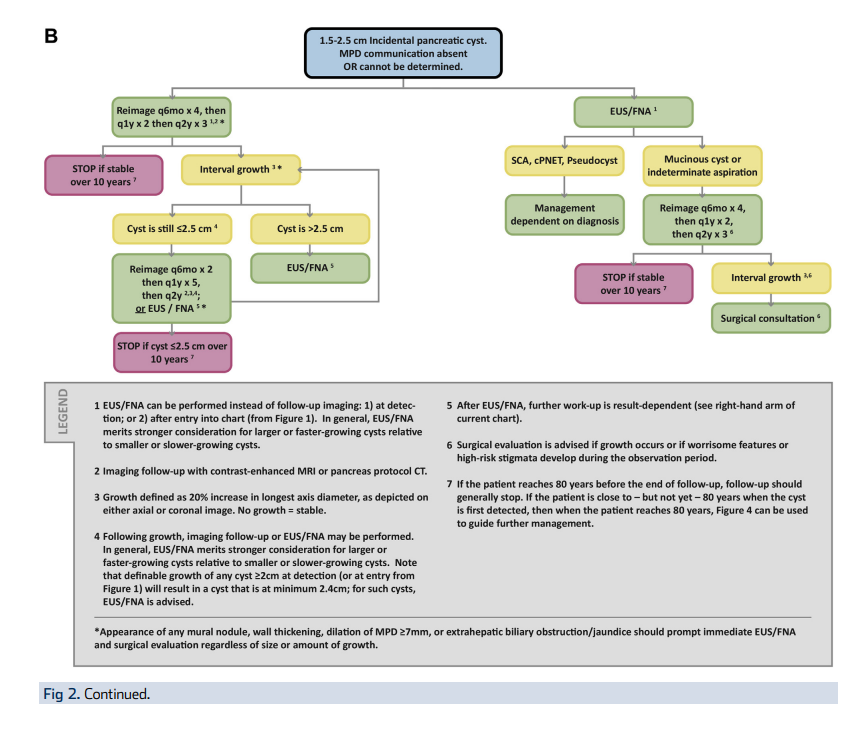
- 2-3 cm: closer imaging, often annually; low threshold for EUS if presumed branch-duct IPMN or if growth develops.
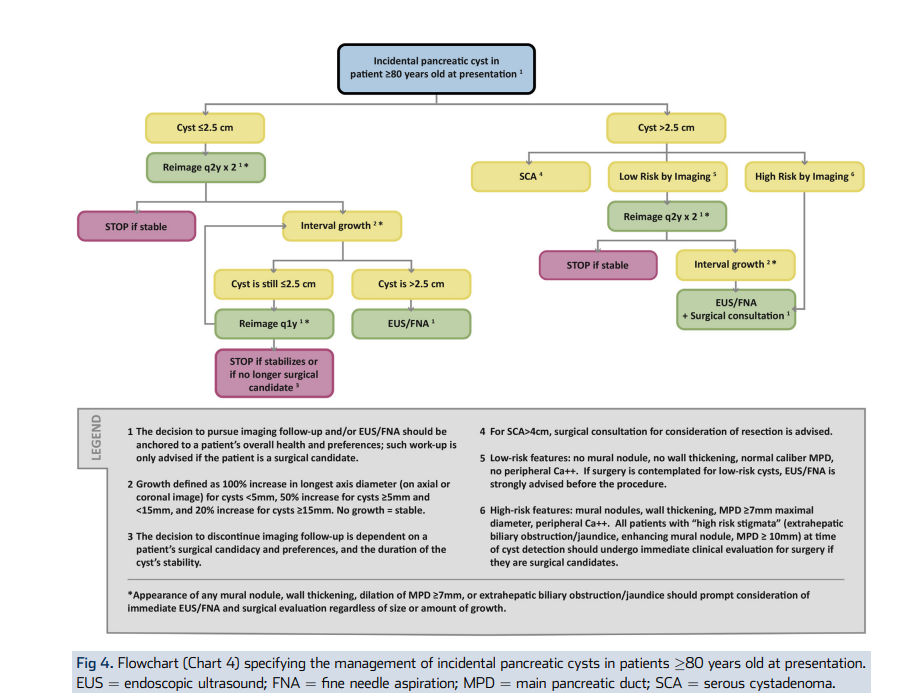
- Consider stopping surveillance when the patient is no longer a surgical candidate.
Escalate / refer
- >= 3 cm or any worrisome feature: EUS +/- FNA and shorter interval follow-up.
- Main-duct or mixed-type IPMN, marked duct dilation, obstructive jaundice, or enhancing nodule/solid component: surgical evaluation if fit.
- Limited life expectancy or poor operative candidacy: avoid intensive prolonged surveillance; individualize follow-up.