Incidental Renal Lesions
Quick Reference Images
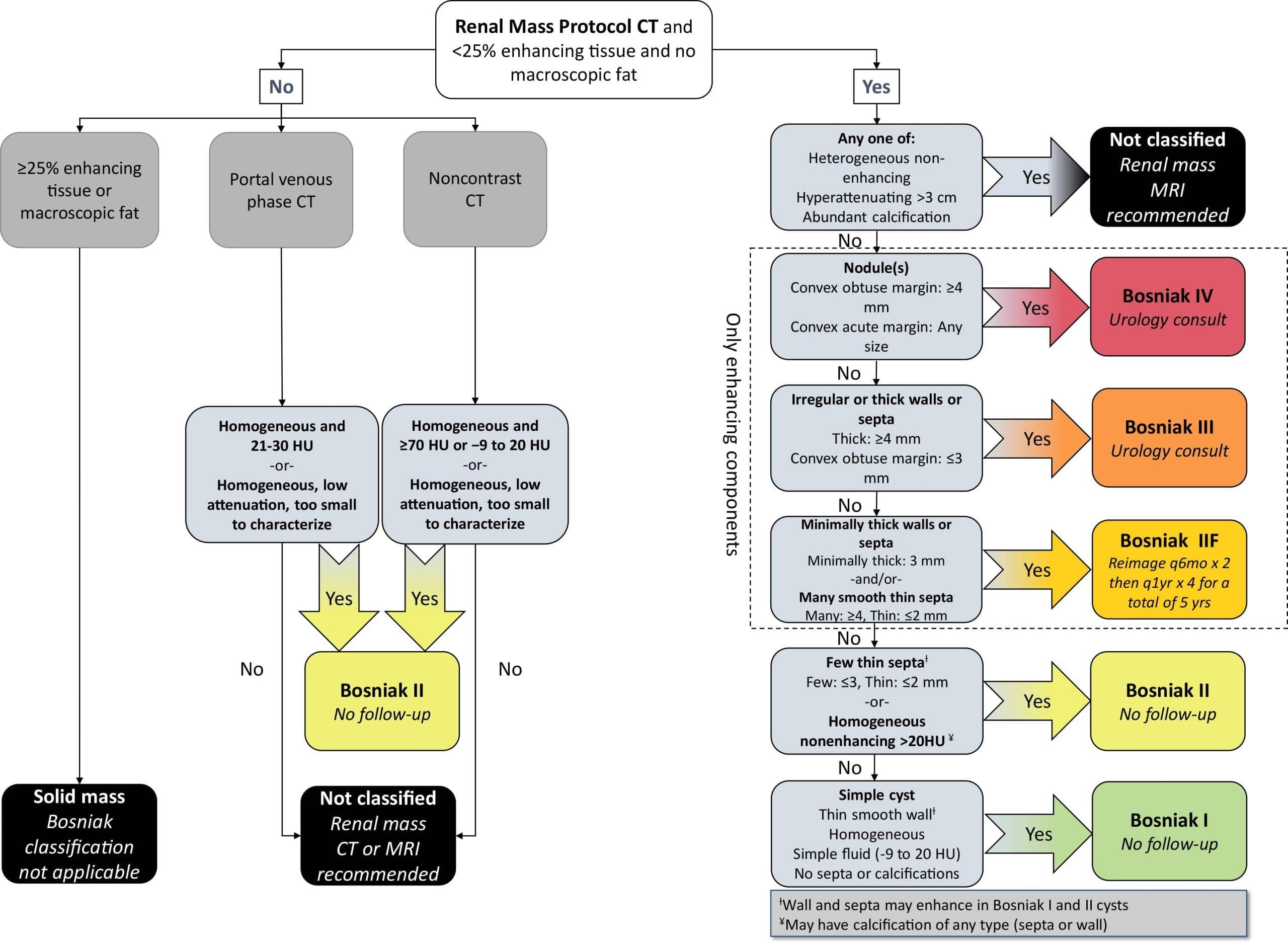
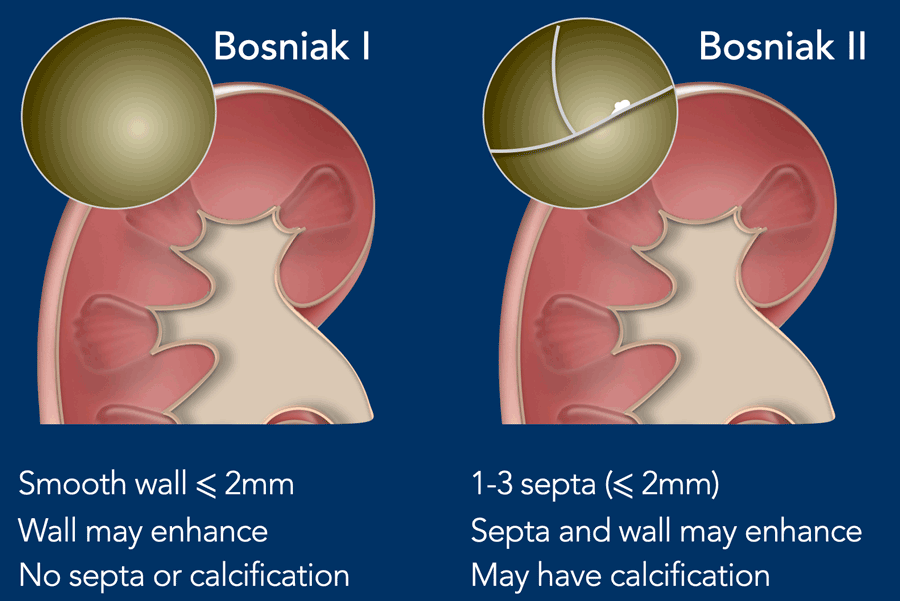
Cystic Lesions
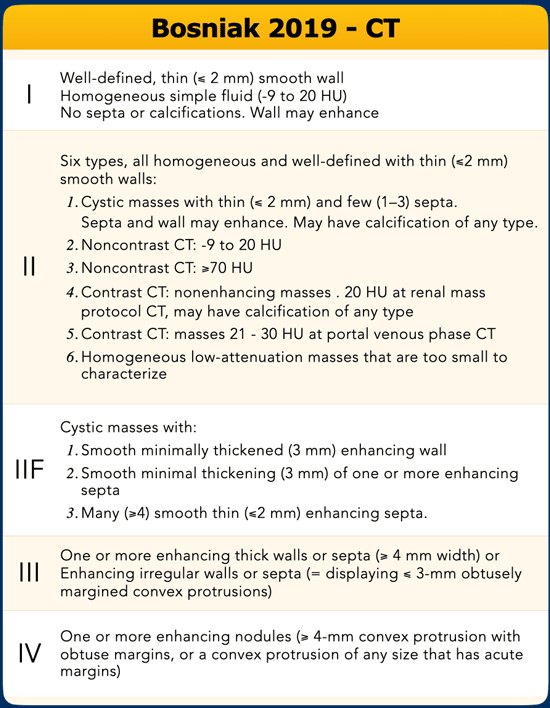
Bosniak I / II
Benign. No imaging follow-up.
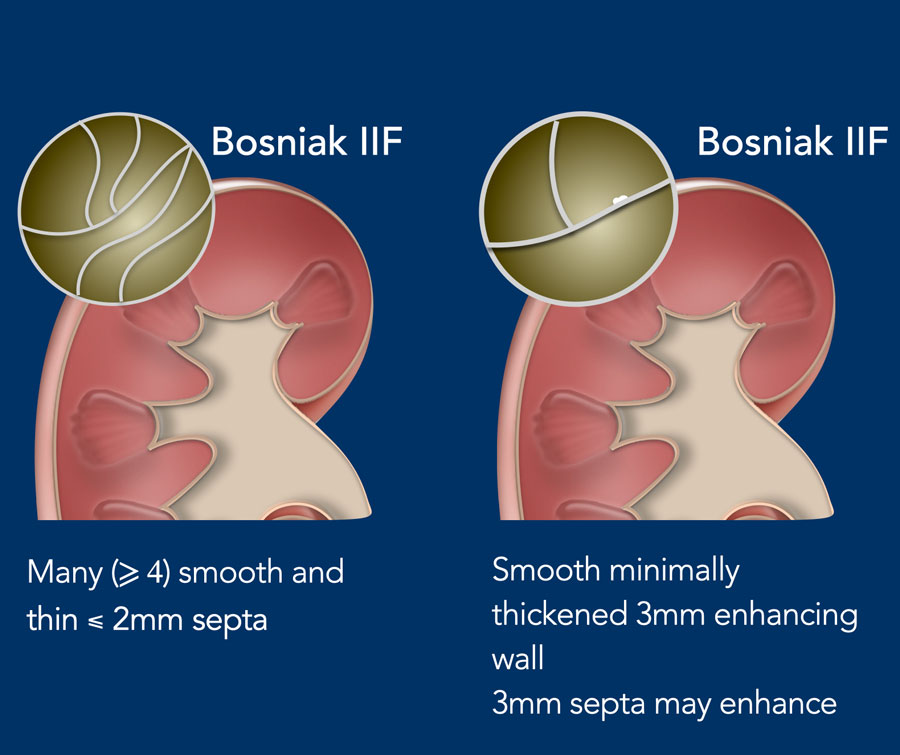
Bosniak IIF
- Low but non-negligible malignancy risk.
- Typical surveillance: repeat CT or MRI at 6 months twice, then yearly for a total of about 5 years.
- Upgrade if new enhancing thick septa/wall, enhancing nodule, or meaningful morphologic progression develops.
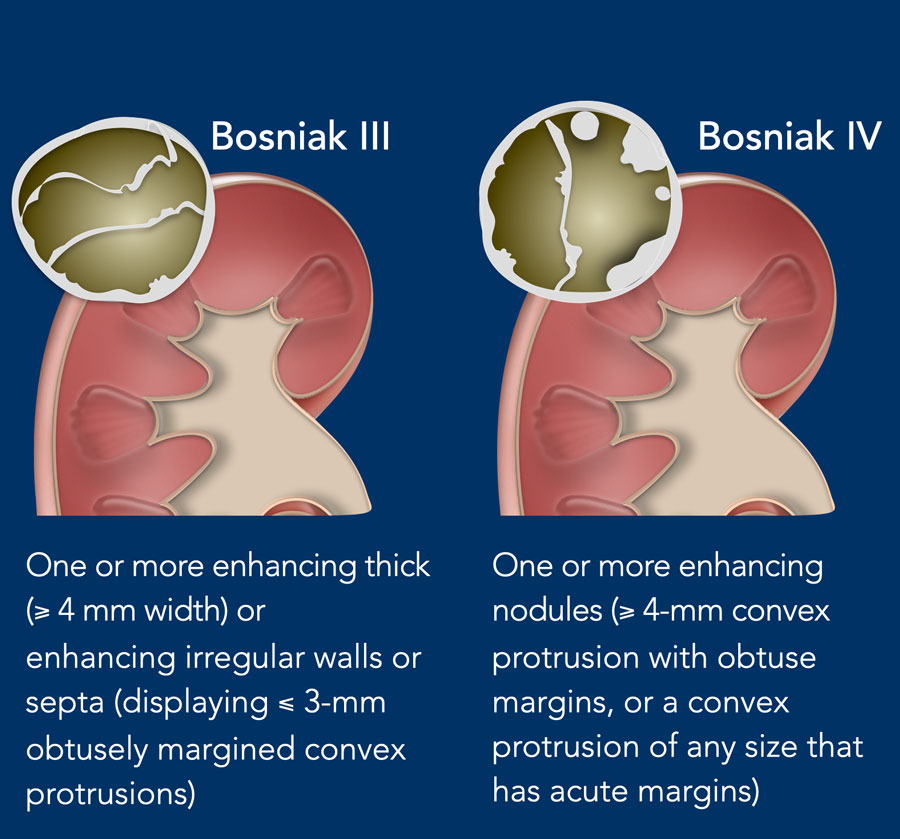
Bosniak III / IV
- Urology consultation is usually appropriate.
- Consider surgery or ablation in fit patients, especially if > 3 cm or morphologically aggressive.
- Management can be individualized in older or comorbid patients.
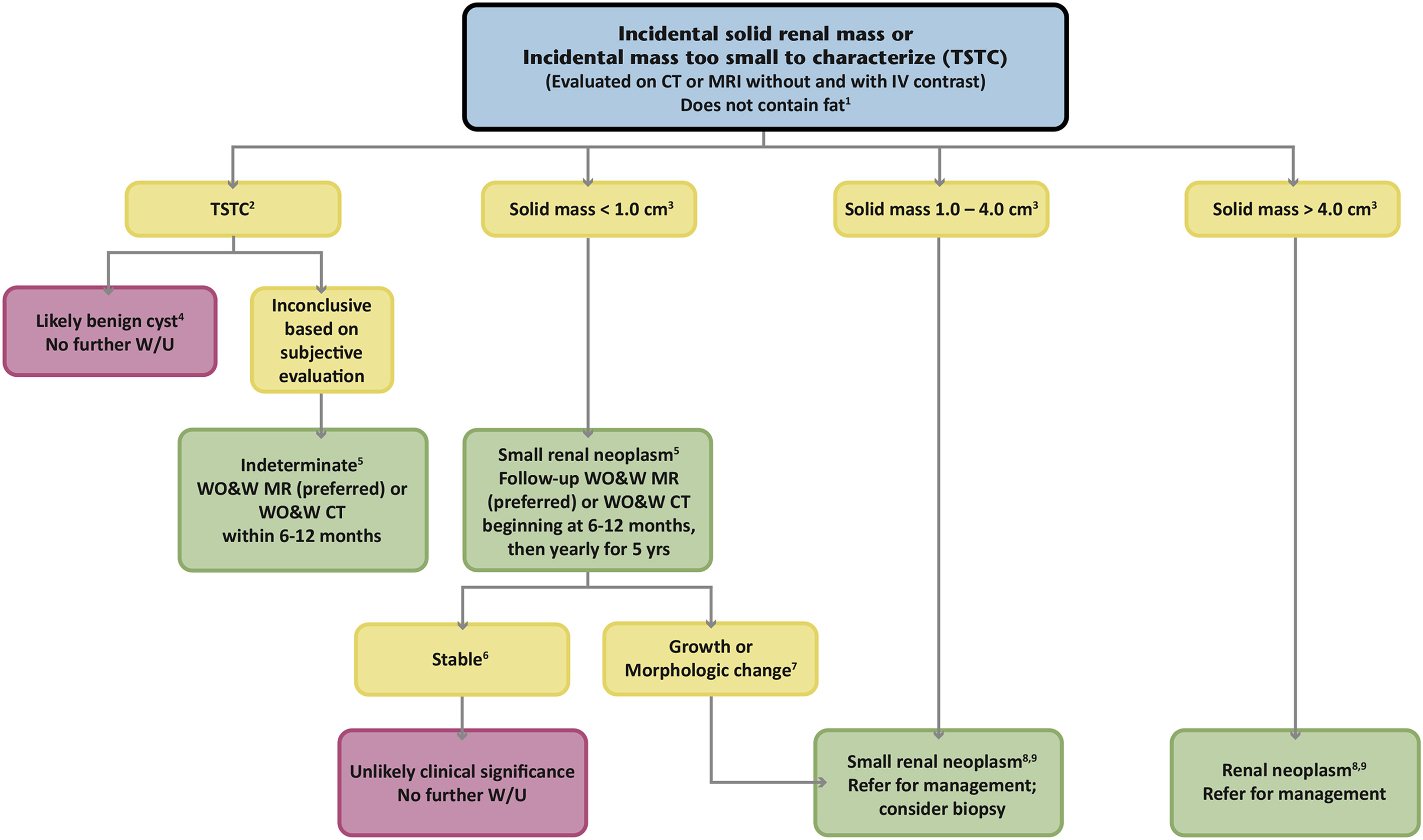
Solid / TSTC
Too small to characterize
- If subjectively likely a benign cyst: no further workup.
- If indeterminate: MRI without and with contrast is preferred; renal mass CT is also acceptable.
- Typical follow-up window for indeterminate TSTC lesions is 6-12 months.
Solid renal mass
- < 1 cm: follow with MRI or CT beginning at 6-12 months, then yearly for about 5 years.
- 1-4 cm: refer for management; consider biopsy depending on imaging and treatment strategy.
- > 4 cm: refer for management.
Growth / morphologic change
Escalate to management referral when a small lesion grows or develops suspicious morphology.
Fat / Protocol / Sources
Fat-containing lesion
- Macroscopic fat strongly suggests angiomyolipoma.
- Fat plus calcification is suspicious for RCC rather than classic angiomyolipoma.
- Larger angiomyolipomas, symptomatic lesions, or lesions with prior hemorrhage may need treatment consideration.
Renal mass protocol
- Use renal mass protocol CT or MRI when enhancement or cyst complexity cannot be assessed on the initial exam.
- Enhancement and Bosniak class drive management for cystic lesions.
- Solid enhancing tissue makes Bosniak classification inapplicable and should be managed as a solid renal mass.