Incidental Splenic Lesions
Reference Images
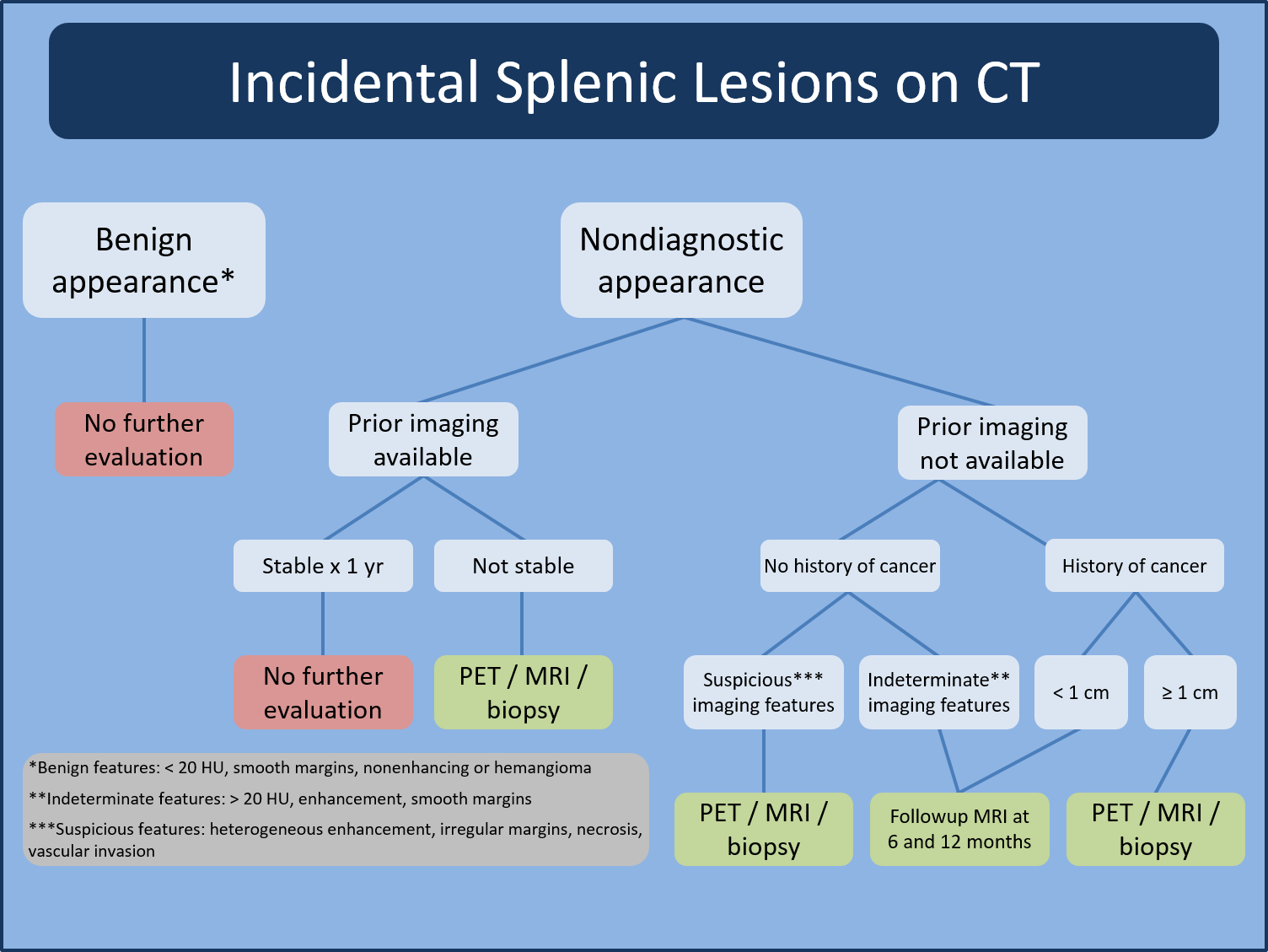
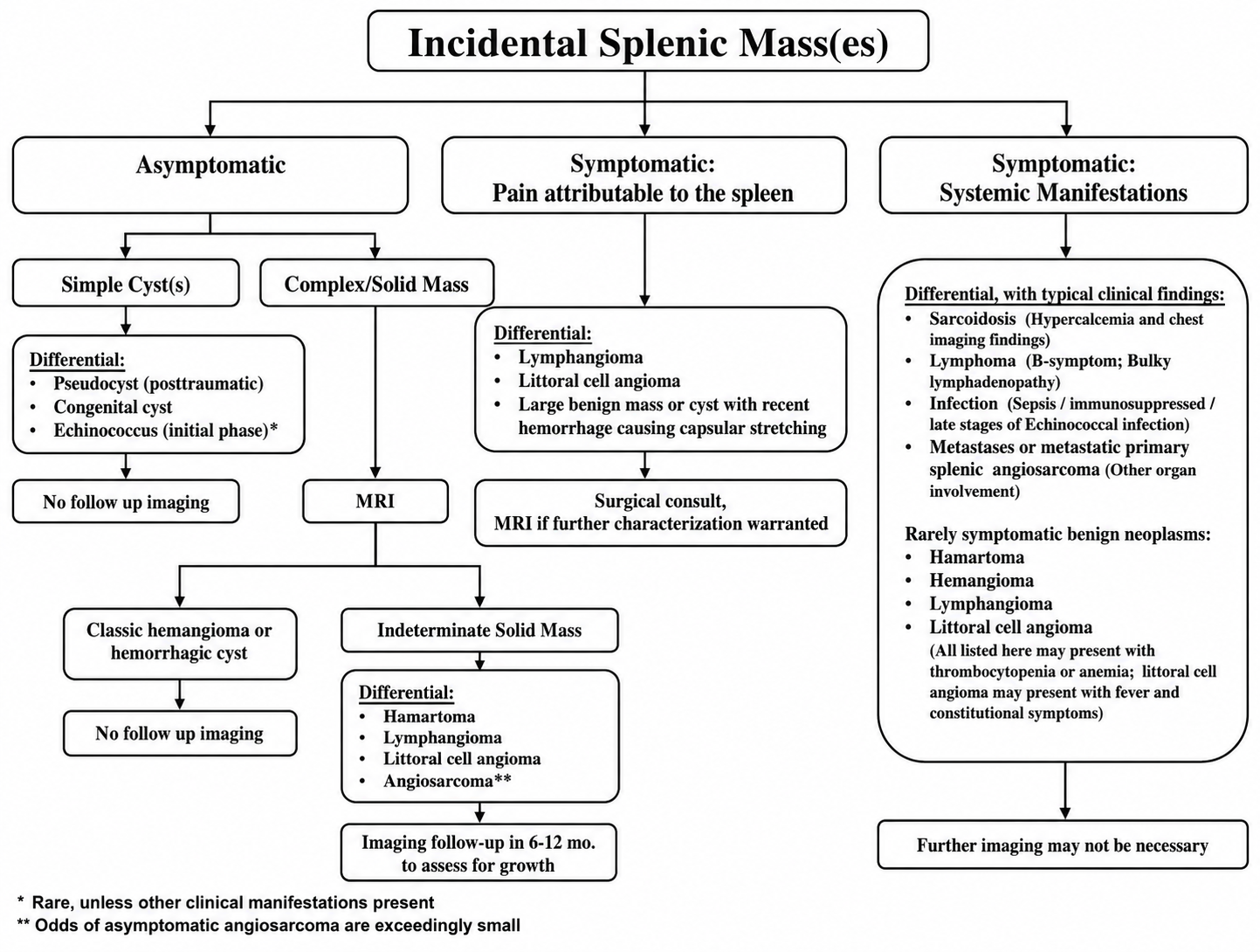
Initial Triage
First question
Benign appearance, prior stability, cancer history, and symptoms drive management more than size alone.
Benign appearance
- Simple cyst, accessory spleen, healed granulomatous calcification, or classic benign vascular lesion: usually no follow-up.
- Benign CT features include smooth margins, homogeneous low attenuation, no enhancement, and no aggressive behavior.
- If a lesion is unchanged for at least 1 year and there is no cancer history, it is generally treated as benign.
Nondiagnostic appearance
- Look for prior imaging first.
- If stable for at least 1 year: no further evaluation.
- If new, enlarging, or no prior comparison: choose follow-up MRI, PET, or biopsy based on cancer history and suspicious features.
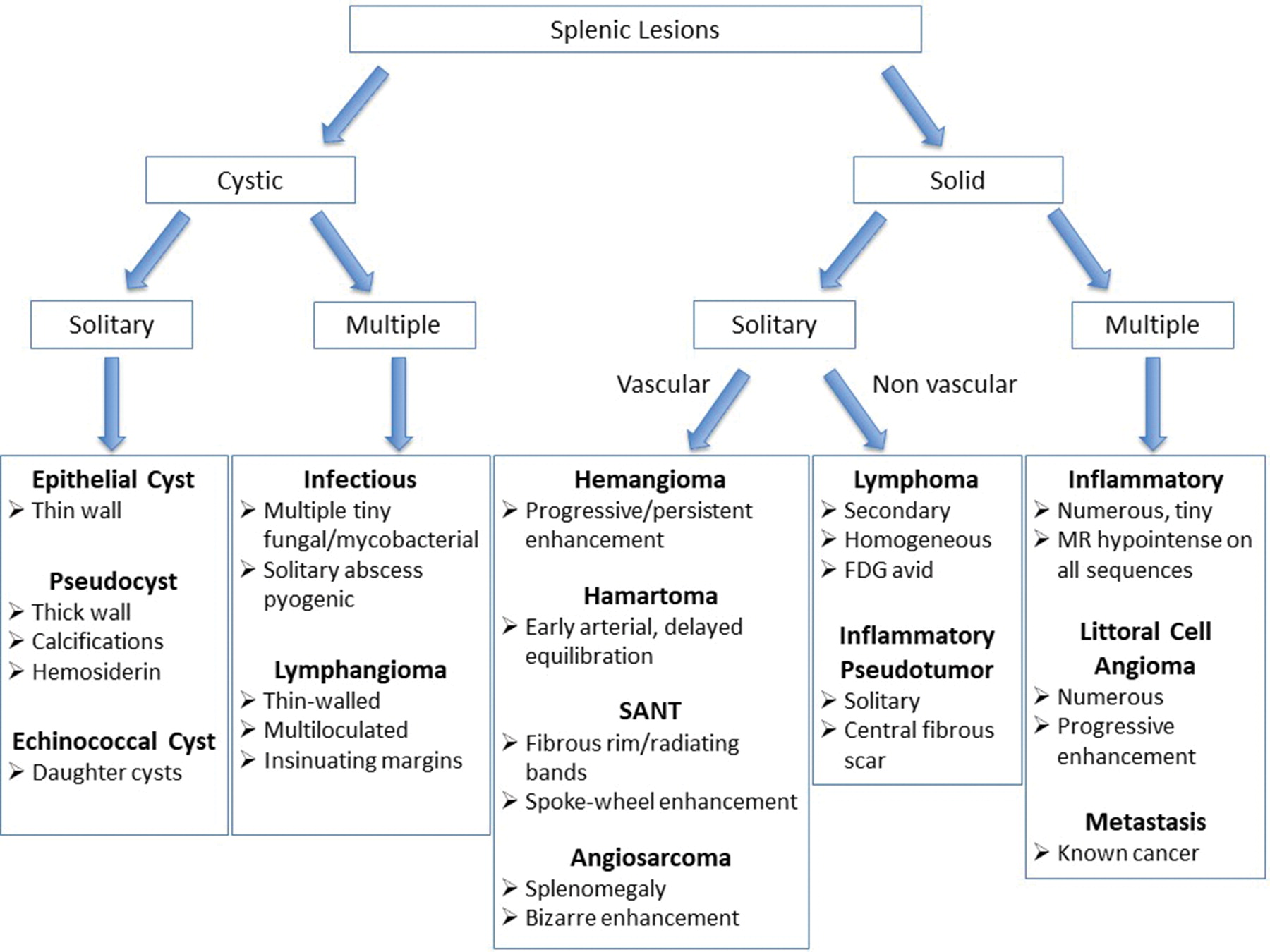
Imaging Patterns
Cystic / benign
- Simple epithelial cyst: thin wall, fluid attenuation/signal, no enhancement.
- Pseudocyst: may have thick wall, calcification, or posttraumatic history.
- Accessory spleen: same enhancement and signal as spleen on every phase/sequence.
Solid vascular / multiple
- Hemangioma: progressive or persistent enhancement.
- Hamartoma: early arterial enhancement with delayed equilibration.
- SANT: fibrous rim/radiating bands or spoke-wheel enhancement pattern.
- Multiple lesions raise inflammatory, lymphoma, littoral cell angioma, or metastasis considerations.
Indeterminate / Suspicious
Escalate
- Suspicious features: heterogeneous enhancement, irregular margins, necrosis, vascular invasion, or rapid growth.
- Known cancer history: lower threshold for MRI, PET, or biopsy, especially for lesions 1 cm or larger.
- No cancer history with indeterminate features: MRI follow-up at about 6 and 12 months is a common pathway.
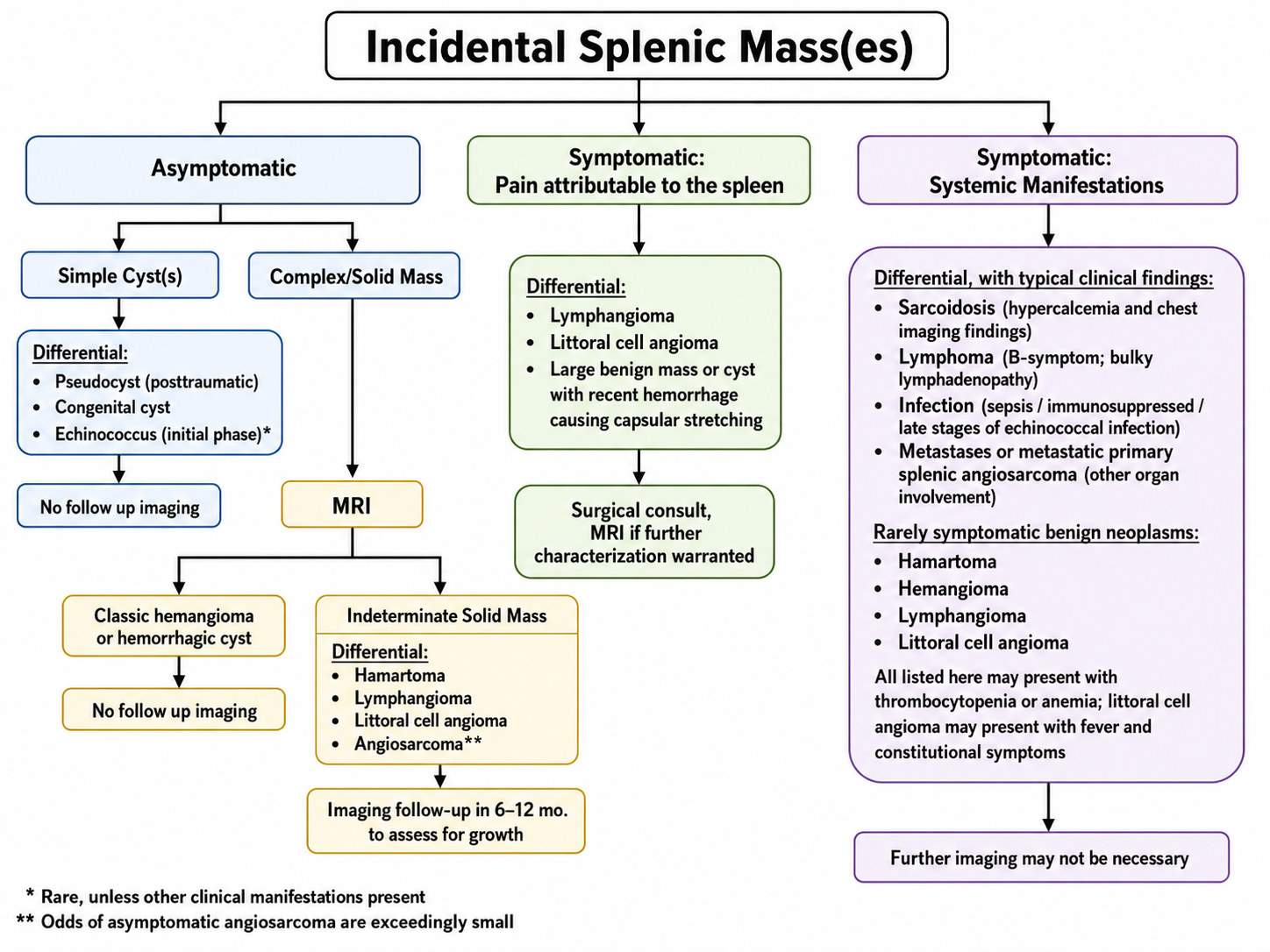
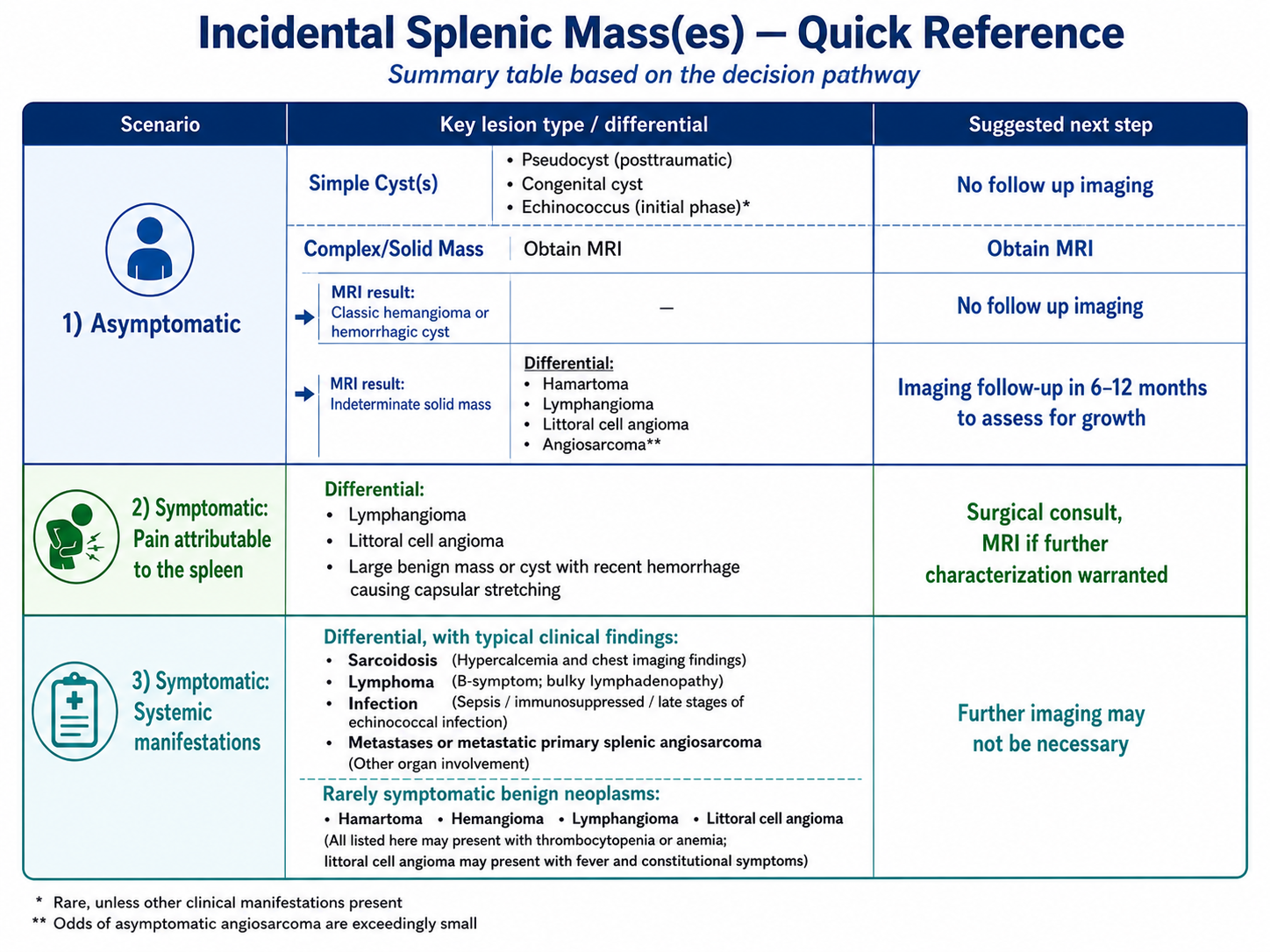
Symptoms
- Pain attributable to the spleen: consider surgical consultation; MRI if further characterization is needed.
- Systemic symptoms or splenomegaly: consider lymphoma, infection, sarcoid, inflammatory disease, metastasis, or angiosarcoma.
- Biopsy is reserved for cases where imaging remains indeterminate and tissue diagnosis will change management.