Thoracic Aortic Aneurysm
Reference Images
Measurement
Most important habit
Measure on double-oblique reformats perpendicular to the vessel long axis, not on routine axial slices.
Technique
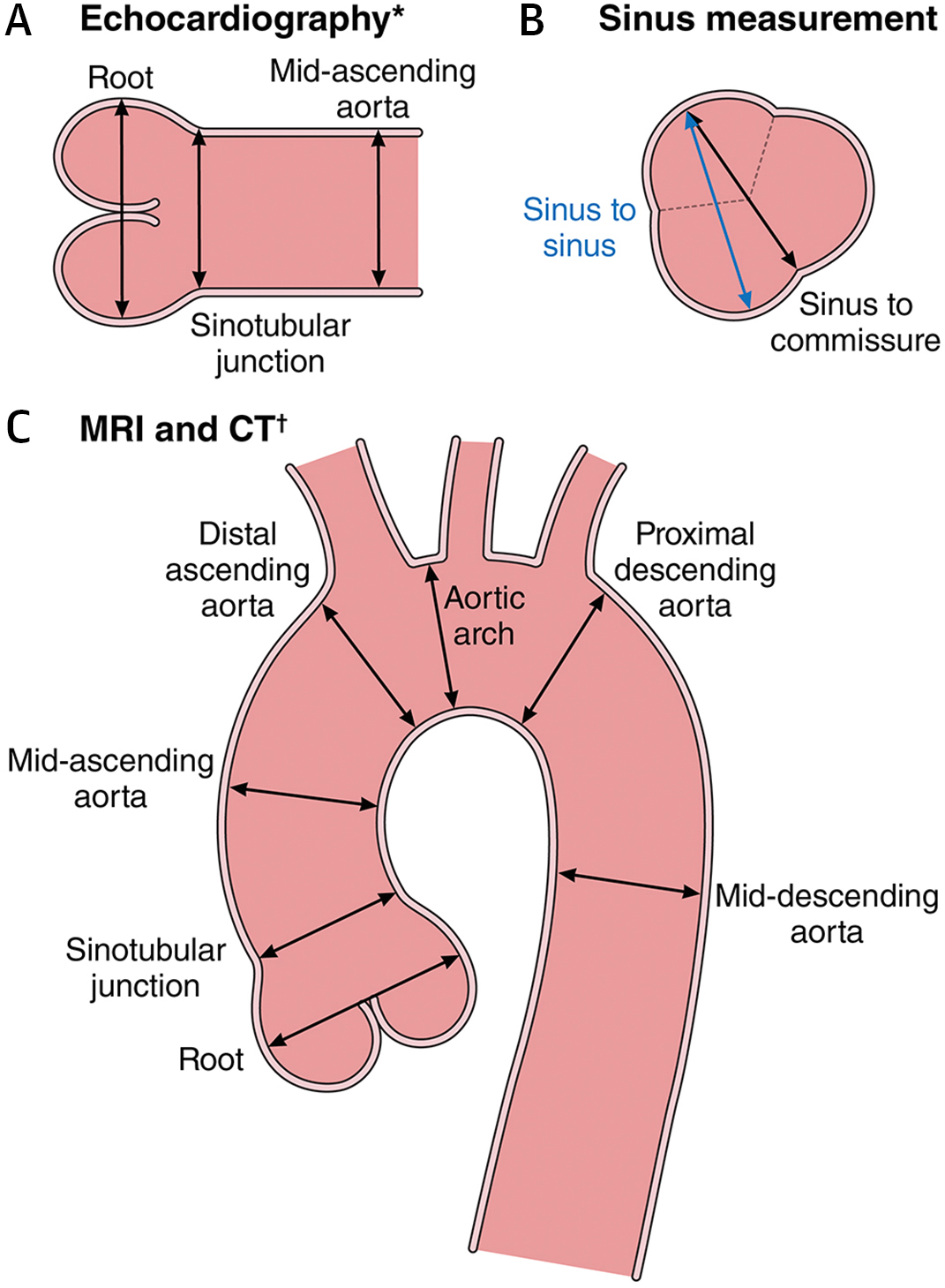
- CT/MRA: outer-wall to outer-wall on centerline or double-oblique multiplanar reformats.
- Root: measure sinus-to-sinus and report the maximum diameter.
- ECG-gating is preferred for the root and ascending aorta; non-gated CT can overestimate by 2-3 mm.
- Avoid cross-modality growth calls when possible because echo, CT, and MRA use different conventions.
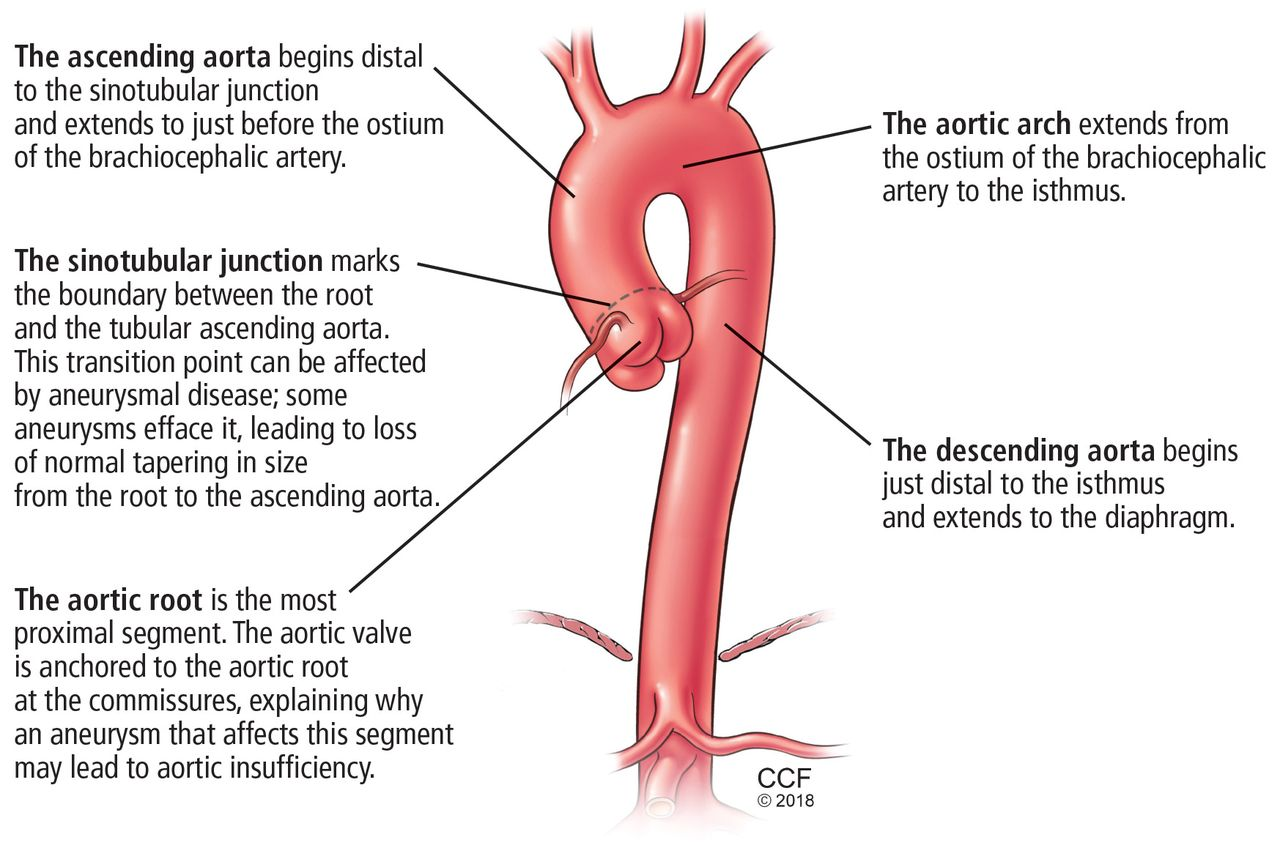
Report landmarks
- Root, sinotubular junction, mid-ascending aorta, arch, isthmus, mid-descending aorta, and diaphragm level.
- State whether the exam was gated and whether measurements are directly comparable to prior imaging.
- Meaningful growth is at least 3 mm, but verify by side-by-side comparison at matched levels.
Surveillance
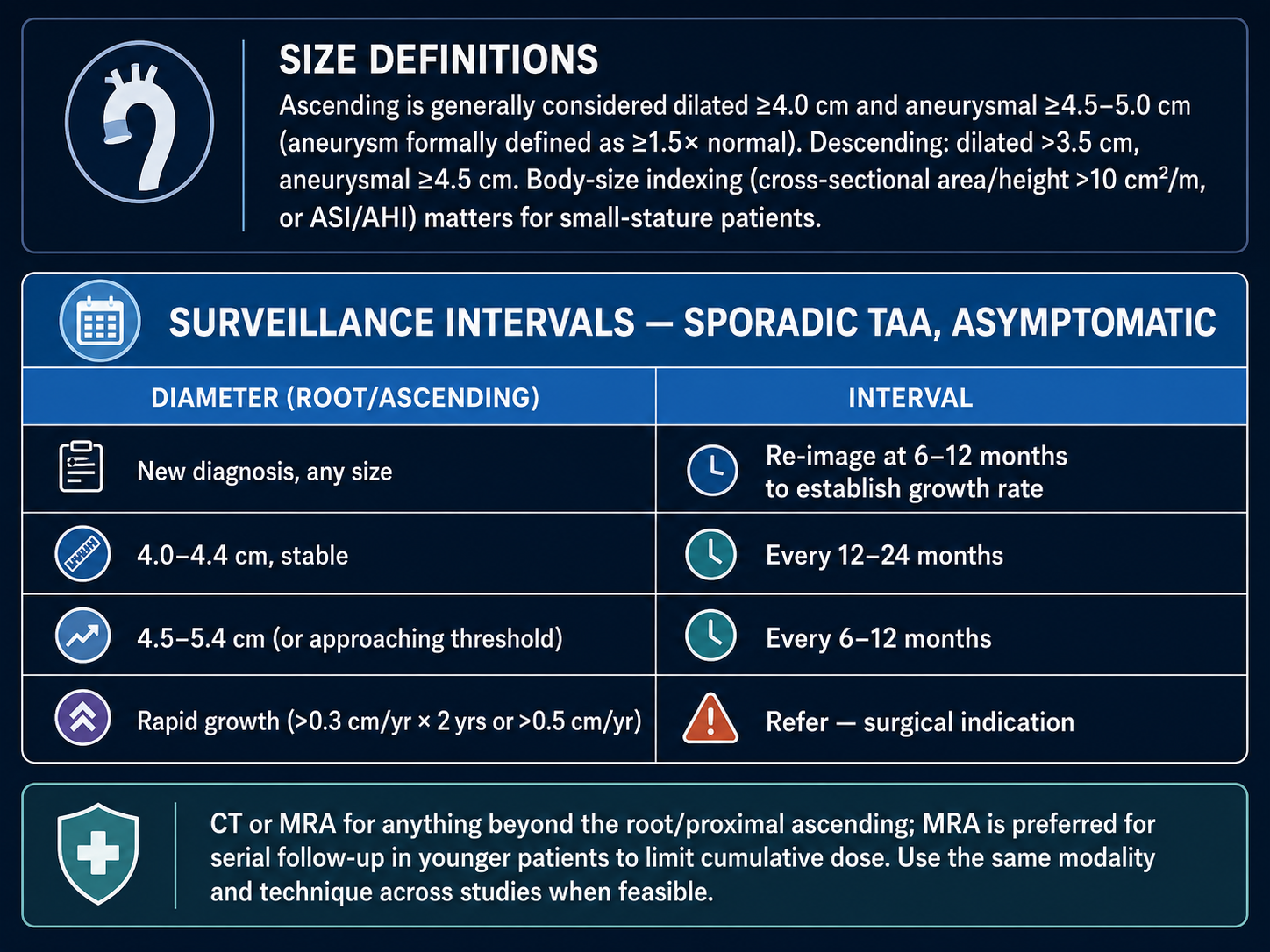
Size definitions
- Ascending aorta: generally dilated at 4.0 cm or greater; aneurysmal at about 4.5-5.0 cm.
- Descending aorta: dilated above 3.5 cm; aneurysmal at 4.5 cm or greater.
- Indexing matters in small-stature patients: cross-sectional area/height greater than 10 cm2/m, ASI, or AHI.
Sporadic asymptomatic TAA
- New diagnosis, any size: re-image at 6-12 months to establish growth rate.
- Root/ascending 4.0-4.4 cm and stable: every 12-24 months.
- Root/ascending 4.5-5.4 cm or approaching threshold: every 6-12 months.
- Rapid growth: refer; surgical indication if at least 0.3 cm/year across 2 years or at least 0.5 cm/year.
Referral / Repair
Thresholds to flag
- Sporadic root/ascending: surgery at 5.5 cm; 5.0 cm is reasonable at experienced aortic centers.
- Bicuspid aortopathy: 5.5 cm; 5.0-5.5 cm with risk factors; 4.5 cm if undergoing aortic valve replacement.
- Marfan: 5.0 cm, or 4.5 cm with risk factors. Loeys-Dietz can be gene-dependent, as low as 4.0-4.5 cm.
- Descending TAA: 5.5 cm; TEVAR preferred when anatomy is suitable, with open repair favored for connective tissue disease.
Post-repair surveillance
- Post-TEVAR: CTA at 1 month and 12 months, then annually if stable. Add 6-month imaging for endoleak or concern.
- Post-open repair: cross-sectional imaging at about 1 year, then roughly every 5 years if stable.
- Include the residual native aorta; watch for endoleak, sac growth, migration, and bird-beaking after TEVAR.