Liver Lesions, HCC Risk / LI-RADS
Reference Images
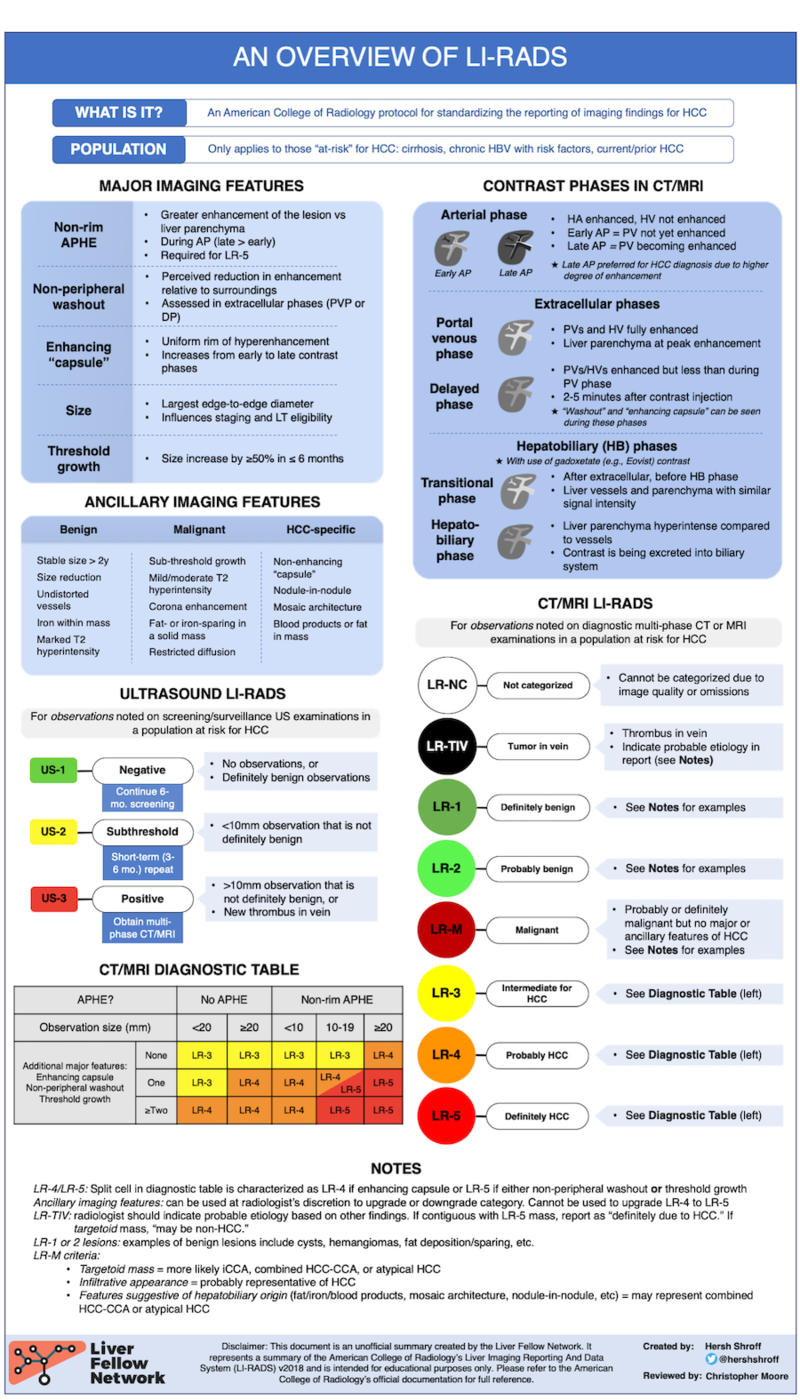
When To Use
Use LI-RADS only in HCC-risk patients.
Cirrhosis, chronic hepatitis B with risk factors, prior HCC, or other accepted HCC surveillance population.
Do not use for
- Otherwise healthy liver with no HCC risk.
- Most noncirrhotic metastatic workups.
- Pediatric patients or uncertain risk status unless the clinical context supports LI-RADS.
Incidental setting
- If a lesion is found on trauma, abdominal pain, or other non-liver protocol CT, first identify whether the patient is HCC-risk.
- If risk is present and the study is not diagnostic, recommend multiphasic liver CT or MRI for LI-RADS categorization.
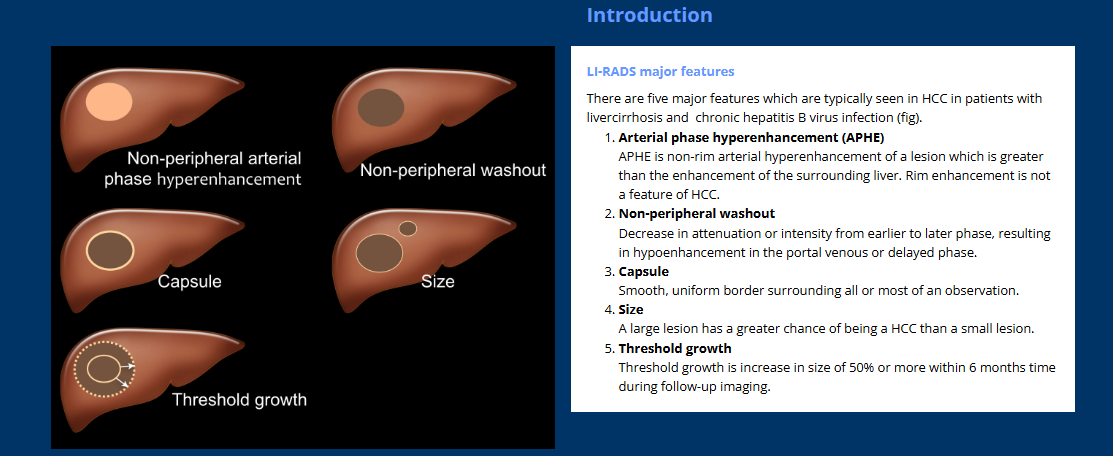
Major Features
Core features
- Non-rim arterial phase hyperenhancement (APHE).
- Non-peripheral washout on portal venous or delayed phase.
- Enhancing capsule appearance.
- Threshold growth.
- Size, especially less than 10 mm, 10-19 mm, and 20 mm or larger.
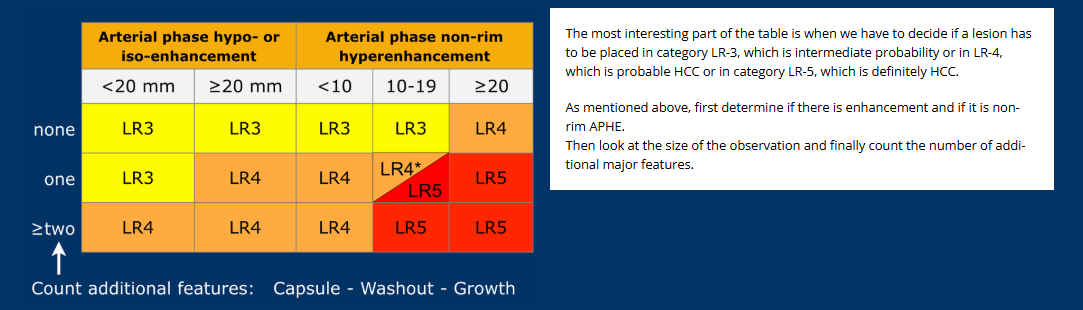
Pattern matters
- Rim APHE favors LR-M rather than classic HCC.
- Non-rim APHE plus size and additional major features drives LR-3 through LR-5.
- Ancillary features may adjust categories but cannot upgrade to LR-5.
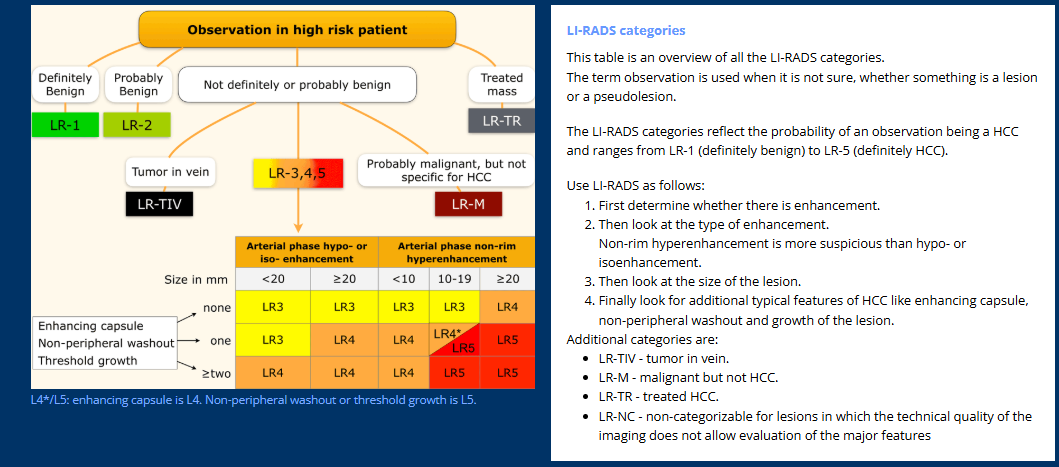
Categories / Action
Diagnostic categories
- LR-1: definitely benign. Continue routine surveillance.
- LR-2: probably benign. Usually routine surveillance.
- LR-3: intermediate probability. Repeat multiphasic CT/MRI, often 3-6 months.
- LR-4: probably HCC. Multidisciplinary review; biopsy, treatment, or very close follow-up.
- LR-5: definitely HCC. Treat/stage as HCC in the right clinical context.
- LR-M: malignant, not specific for HCC. Biopsy or additional workup is usually needed.